
A Federated K-Means-Based Approach in eHealth Domains with
Heterogeneous Data Distributions
Giovanni Paragliola
1 a
, Patrizia Ribino
2 b
and Maria Mannone
2,3 c
1
National Research Council (CNR), Institute for High-Performance Computing and Networking (ICAR), Naples, Italy
2
National Research Council (CNR), Institute for High-Performance Computing and Networking (ICAR), Palermo, Italy
3
Institute of Physics and Astronomy, University of Potsdam, Potsdam, Germany
{giovanni.paragliola, patrizia.ribino, maria.mannone}@icar.cnr.it
Keywords:
Federated Clustering, Healthcare, Heterogeneous Data Distribution.
Abstract:
Healthcare organizations collect and store significant amounts of patient health information. However, sharing
or accessing this information outside of their facilities is often hindered by factors such as privacy concerns.
Federated Learning (FL) data systems are emerging to overcome the siloed nature of health data and the
barriers to sharing it. While federated approaches have been extensively studied, especially in classification
problems, clustering-oriented approaches are still relatively few and less widespread, both in formulating al-
gorithms and in their application in eHealth domains. The primary objective of this paper is to introduce a
federated K-means-based approach for clustering tasks within the healthcare domain and explore the impact of
heterogeneous health data distributions. The evaluation of the proposed federated K-means approach has been
conducted on several health-related datasets through comparison with the centralized version and by estimating
the trade-off between privacy and performance. The preliminary findings suggest that in the case of hetero-
geneous health data distributions, the difference between the centralized and federated approach is marginal,
with the federated approach outperforming the centralized one on some healthcare datasets.
1 INTRODUCTION
Healthcare organizations typically gather large
amounts of patient health data. Multi-centre research
plays a crucial role in developing machine learning
(ML) algorithms for real-world scenarios. However,
various factors hinder the dissemination or retrieval
of this information outside the organization, such
as privacy concerns (Bonawitz et al., 2021). The
Health Insurance Portability and Accountability Act
(HIPAA) (Act, 1996) and the General Data Protection
Regulation (GDPR) (Voigt and Von dem Bussche,
2017) have established regulations that restrict the ex-
change of electronic health records (EHRs) between
stakeholders and healthcare providers without patient
consent (Sheller et al., 2020). Protecting confidential
medical information while leveraging the collective
knowledge of healthcare facilities presents a complex
and demanding challenge (Dhade and Shirke, 2024).
Federated Learning (FL) systems are emerging as
a
https://orcid.org/0000-0003-3580-9232
b
https://orcid.org/0000-0003-3266-9617
c
https://orcid.org/0000-0003-3606-3436
a promising solution to overcome the siloed nature of
health data and the associated barriers to sharing them
(Bharati et al., 2022). FL enables the decentralized
training of ML models without transferring medical
data to a central server. Each healthcare institution
is a client node, which independently trains its model
and transmits it to a central server for aggregation.
A global model is formed by integrating local mod-
els from all nodes, which are then disseminated to the
nodes by a centralized server responsible for coordi-
nating and aggregating the models.
However, while federated approaches have been
extensively studied, mainly in the context of classifi-
cation problems (Marulli et al., 2021a; Marulli et al.,
2021b), clustering-oriented approaches remain rela-
tively scarce and less widespread. The formulation
of algorithms tailored explicitly for federated cluster-
ing and their application in e-health domains are areas
that are still in their early stages of exploration.
Despite the benefits of federated learning, such as
preserving privacy and reducing communication over-
head, a more comprehensive investigation is required
to fully understand and leverage the advantages of
federated clustering in healthcare domains. As the
550
Paragliola, G., Ribino, P. and Mannone, M.
A Federated K-Means-Based Approach in eHealth Domains with Heterogeneous Data Distributions.
DOI: 10.5220/0012981200003837
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 16th International Joint Conference on Computational Intelligence (IJCCI 2024), pages 550-559
ISBN: 978-989-758-721-4; ISSN: 2184-3236
Proceedings Copyright © 2024 by SCITEPRESS – Science and Technology Publications, Lda.

healthcare landscape evolves toward more collabora-
tive and data-driven models, addressing these issues
will become increasingly critical to realizing the full
potential of federated learning to improve patient out-
comes and advance medical research.
Furthermore, when investigating methodologies
for distributed clustering, it is imperative to con-
sider the distinct challenges associated with federated
learning, such as data heterogeneity, meaning that
data are not uniformly distributed among the partic-
ipants. This problem, known as the non-independent
and identically distributed (non-IID) data challenge
(Wahab et al., 2021), occurs when the local data of
individual clients does not accurately reflect the en-
tire dataset due to heterogeneous class imbalances,
distribution variations, and data size. These chal-
lenges can lead to significant performance degrada-
tion in federated learning models because traditional
machine learning algorithms assume uniform data
distribution across clients. In particular, local updates
may diverge during model aggregation, resulting in
slow convergence or even degraded performance in
the global model. To address these issues, various
strategies have been proposed, including methods for
grouping clients with similar data distributions. These
weighted aggregation schemes assign importance to
clients based on data size or distribution and fine-
tuning global models on local data.
This paper presents a study focused on evaluating
a federated clustering approach in the e-health domain
in non-IID scenarios. Specifically, the primary objec-
tive is to introduce a federated K-means-based (FKM)
approach for clustering within the healthcare domain
and explore the impact of heterogeneous data distri-
butions. The evaluation of the proposed approach
has been conducted on several health-related datasets
through comparison with the centralized version and
by estimating the trade-off between privacy and per-
formance. The approach was evaluated mainly un-
der three different data distribution scenarios to more
accurately assess the impact of data heterogeneity
across clients on the federated model. These scenar-
ios range from independent and identically distributed
data across clients to a non-independent and iden-
tically distributed scenario, within which we distin-
guish soft and hard heterogeneity.
The preliminary findings suggest that in the case
of heterogeneous health data distributions, the differ-
ence between the centralized and federated approach
is marginal, with the federated approach outperform-
ing the centralized one on some healthcare datasets.
The paper’s contribution can be summarized into
two main points: 1) Establish a federated K-means
approach to evaluate the effectiveness of clustering
models in the federated eHealth domain; 2) Inves-
tigate how the hypothesis of heterogeneous health
data distribution affects the convergence of local and
global models.
2 RELATED WORKS
Centralized clustering approaches require storing and
accessing all raw data from a single central node. The
K-means clustering algorithm, introduced more than
six decades ago, continues to be widely favored and
utilized in contemporary research and practice.
Federated clustering is a framework within the
field of federated learning whose objective is to clus-
ter data distributed across multiple devices or loca-
tions while preserving privacy and data security. The
process involves aggregating local data points that
exhibit global similarity. The distributed nature of
the data points allows for their clustering based on
a global similarity measure, as they are distributed
among multiple clients. Notably, the data remains lo-
cal on client devices despite the clustering process.
Based on our current understanding, a limited body
of literature is devoted to investigating this issue.
Federated K-means clustering can be used to per-
form unsupervised learning (for a variable number of
clusters between centers), also clustering on multiple
datasets avoiding sharing the underlying data (Garst
and Reinders, 2024). The idea of avoidance of lo-
cal, sensitive data sharing is also used in the algo-
rithm for Federated, Fair, and Fast K-means (F
3
KM)
(Zhu et al., 2023). With this approach, the K-means
are efficiently solved in vertical FL. The overall prob-
lem is decomposed into multiple sub-problems that
are solved at the level of single clients. Thus, the
clients only transmit their results to the server rather
than the original sensitive data. Clustering precision
may be enhanced by exploiting local data stored on
each client to help define better initial centroids (Yang
et al., 2024). Defining the initial centroids directly
at the server level results in the initial features be-
ing devoid of insights derived from the clients. Then,
the server finds the initial global centroids, feeding a
greedy algorithm with the client-based information.
To improve the first step, the clients share the data
point number for each centroid, allowing better parti-
tioning. The problem of privacy and security in FL
is addressed in (Pedrycz, 2022) using fuzzy logic,
and in particular, a problem of unsupervised feder-
ating learning is solved via fuzzy sets based on fed-
erated clustering, named Fuzzy C-Means Federated
(F-FCM). In (Pedrycz, 2022), an objective function is
proposed. Clusters are formed via a partition function
A Federated K-Means-Based Approach in eHealth Domains with Heterogeneous Data Distributions
551

that assigns points to them, and a set of cluster proto-
types is updated according to the exchanges between
the server and clients. Another fuzzy approach is used
for multistep federated clustering, validating clusters
through the DB index (Stallmann and Wilbik, 2022).
An alternative methodology addressing the pri-
vacy concerns associated with FKM within proac-
tive caching for cellular networks is put forth by (Liu
et al., 2020). The base stations collect users’ data,
which may cause an information leakage. The so-
lution of (Liu et al., 2020) uses privacy-preserving
federated K-means and secret-sharing protocols. The
passage of secret sharing is needed to avoid recon-
structing users’ data from the shared gradients up-
loaded to the macro-cell base station to update cluster
centroids. Splitting the gradient into random shared,
its reconstruction is only made possible when a mini-
mal number of the shared is collected, thus guarantee-
ing the privacy of user data. Moreover, secure aggre-
gation and homomorphic encryption strategies mak-
ing K-means more robust concerning non-IID data
(nonindependent and identically distributed) are ad-
dressed in (Brand
˜
ao et al., 2021).
The current study introduces a novel K-means ap-
proach based on a global centroids similarity measure
to improve the balance between maintaining privacy
and achieving effective clustering. We start with the
standard K-means clustering steps and add modifica-
tions to integrate them with federated learning. Addi-
tionally, our study explores the potential influence of
the heterogeneous health data distribution on the con-
vergence of local and global models using real-world
healthcare datasets.
3 MATERIALS AND METHODS
3.1 Federated K-Means Approach
Beyond the aforementioned advantage concerning
privacy issues, we focus on federated clusters for
their multiple benefits. To name but a few, we
mention their scalability efficiency (no need to store
and process the whole dataset in the same location),
data control (to remain in possession of individual
clients), and communication efficiency (reduction of
the amount of shared data). Other advantages in-
clude decreased large-scale data breaches, real-time
latency reduction, and local pattern discovery. This
last element is particularly relevant in medical ap-
plications. The investigation of heterogeneously-
distributed medical datasets is, in fact, the primary
motivation of our research.
The main steps of the federated K-means algo-
rithm presented here are the following: In the first
phase, (Broadcast Parameters), the central server pro-
vides the different clients with training parameters,
including the number of clusters to set for each lo-
cal model, the maximum number of iterations, and
the centroid initialization method. After this phase,
each client independently performs clustering by ap-
plying the K-means algorithm to its data. Each client
transmits its set of centroids to the central server (Col-
lect Local Centroids), randomly selecting a set of cen-
troids from one of the n clients (Random Selection
of Centroid C
∗
), hereinafter referred to as C
∗
, indi-
cating the initialization set of centroids to define the
global centroids. Indeed, the global centroids defi-
nition needs an initialization of centroids’ selections
as the local K-means; the selection of C
∗
addresses
this requirement. Then, for each centroid c belong-
ing to C
∗
, the central server creates a set of centroids
belonging to other clients closest to cosine similarity
according to the following formula:
∀c ∈ C
∗
, S
c
= min
j
(cosine(c, c
i j
)), (1)
where C
∗
is the initial set of centroids for the defini-
tion of global centroids, c is the generic centroid be-
longing to C
∗
, and S
c
is the set of the closer centroids
to c belonging to C
j
, with C
j
̸= C
∗
.
After identifying for each centroid c ∈ C
∗
the cor-
respondence set S
c
, the global centroids are computed
as the average (Calculate global centroids). At this
point, local centroids are evaluated and sent to local
nodes (Broadcast global centroids), which repeat the
local clustering until the rounds are completed.
3.2 Datasets
The following four publicly available datasets and a
synthetic dataset are used to evaluate the FKM model:
• OASIS2 (Battineni et al., 2019) is a dataset re-
lated to Alzheimer’s disease (AD) containing pa-
tient sociodemographic characteristics and clini-
cal variables. Size: 354 samples x 12 features.
• Heart Disease (Abid Ali Awan, 2021) is a dataset
with features of heart disease patients. Size: 303
samples x 11 features.
• Obesity (Palechor and De la Hoz Manotas, 2019)
is a dataset containing data to estimate obesity in
patients according to their eating habits and phys-
ical condition. Size: 2111 samples x 17 features.
• Breast Cancer (W. H. Wolberg and Mangasarian,
2017) is a dataset of digitized images of fine nee-
dle aspirates from breast masses. Size: 569 sam-
ples x 30 features.
NCTA 2024 - 16th International Conference on Neural Computation Theory and Applications
552
• Custom is a synthetic dataset. Size: 500 samples
x 10 features.
3.3 Data Distribution Scenarios
The data contained in each dataset have been used to
define three scenarios corresponding to three differ-
ent data distributions. Specifically, we define a uni-
form distribution, where the data are uniformly dis-
tributed between clients; a soft-heterogeneous distri-
bution, which exhibits a slight heterogeneity of data
distribution; and finally, a hard-heterogeneous distri-
bution, which is characterized by a pronounced het-
erogeneity of data distribution. Each scenario repre-
sents a different usage context for our model and will
allow us to evaluate its performance under realistic
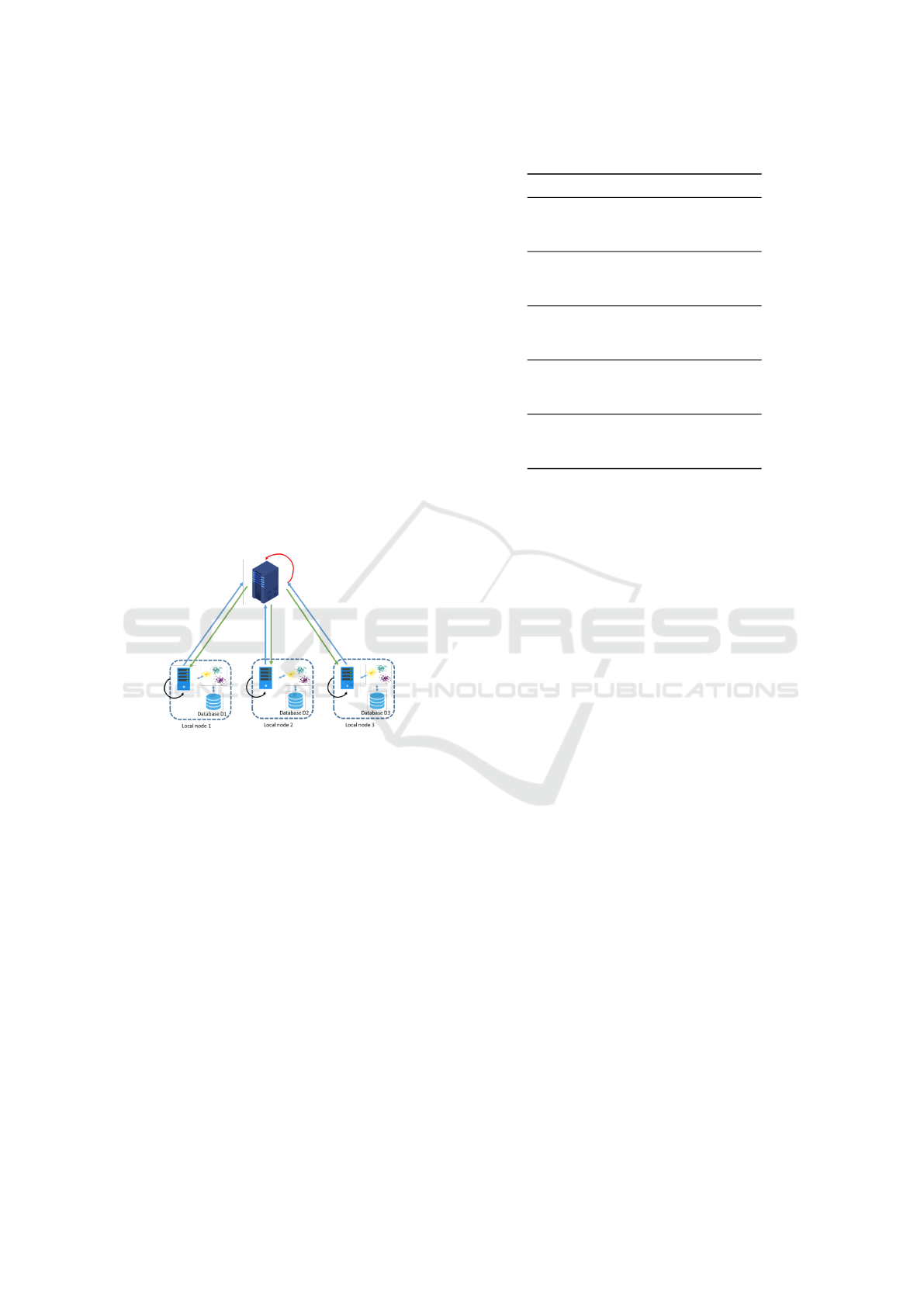
and varied conditions. Figure 1 shows the architec-
ture used for the Federated Clustering. It is delineated
by two primary nodes: local nodes, also known as
client nodes, and server nodes, which act as aggrega-
tors. Without loss of generality, we assume to work
with three client nodes and one aggregator node.
Figure 1: Federated architecture with 3 client nodes.
The clients emulate three entities where data are
stored and are subject to mobility constraints to facili-
tate machine-learning training. The aggregator serves
as the focal point for the aggregation process, receiv-
ing the local centroids generated by the clients during
each round of communication.
In each of the three considered scenarios, each
client stores a data portion according to a type of het-
erogeneous data distribution (HDD), as follows: (i)
Homogeneous (H)- Each client has the same number
of samples; (ii) Soft-Heterogeneous (SH)- Each sam-
ple in the dataset is randomly assigned to one of the 3
clients according to a uniform distribution; (iii) Hard-
Heterogeneous (HH)- First, 80% of each dataset is
equally distributed among all clients. Then, half of the
clients are randomly selected to receive the remaining
20% of the data, again using a uniform distribution.
A sample allocation example is shown in Table 1.
It is worth introducing the hypothesis underlying
Table 1: Client’s samples for each dataset.
Client Datatet H SH HH
1 OASIS2 118 108 165
2 OASIS2 118 138 98
3 OASIS2 118 108 91
1 Heart Disease 101 105 146
2 Heart Disease 101 105 63
3 Heart Disease 101 93 94
1 Obesity 703 664 1003
2 Obesity 703 731 568
3 Obesity 703 716 540
1 Breast Cancer 189 176 238
2 Breast Cancer 189 166 135
3 Breast Cancer 189 158 127
1 Custom 166 173 257
2 Custom 166 201 173
3 Custom 166 195 139
our proposed approach. Since we are defining our use
case in a federated environment with multiple clients,
each client performs independent local clustering on
its data. To compare clustering results across clients,
we assume that the probability distributions on the lo-
cal clients are identical. This assumption implies that
the underlying probability distributions governing the
data points are consistent across clients:
F
X
(x) = F
Y
(x) ∀x ∈ X with X ̸= Y, (2)
where F is the probability distribution function, and
X and Y are two generic clients. By assuming the
same probability distribution, the comparison of the
clusters produced by different clients becomes mean-
ingful. Consequently, we can evaluate the effective-
ness and consistency of the clustering algorithms em-
ployed across the distributed system.
4 COMPARISON BETWEEN
CENTRALISED AND
FEDERATED K-MEANS
We perform a comparative analysis from two perspec-
tives to evaluate the proposed federated K-means ap-
proach. First, we compare the performance of the two
approaches using widely known metrics for unsuper-
vised techniques, assessing the quality and effective-
ness of the clustering algorithms. Then, we compare
the two approaches considering cluster composition
and the similarity of items within clusters.
Experiments were conducted to evaluate different
cluster configurations, with cluster numbers ranging
from two to five. A random initialization was used
alongside a max iteration parameter set at 100.
A Federated K-Means-Based Approach in eHealth Domains with Heterogeneous Data Distributions
553
Table 2: Overview of the Performance Results - Hard Heterogeneous Distribution.
Dataset Clusters Approach Silhouette
Calinski
Harabasz
Davies
Bouldin
Approach Silhouette
Calinski
Harabasz
Davies
Bouldin
oasis2 2 Centralized 0.19 76.40 2.00 Federated 0.19 73.63 2.06
oasis2 3 Centralized 0.20 71.87 1.80 Federated 0.26 93.52 1.58
oasis2 4 Centralized 0.26 87.22 1.53 Federated 0.40 141.77 1.27
oasis2 5 Centralized 0.44 143.20 1.13 Federated 0.61 238.33 1.05
ObesityDataSet 2 Centralized 0.19 277.98 2.53 Federated 0.11 225.02 2.92
ObesityDataSet 3 Centralized 0.12 228.80 2.37 Federated 0.34 174.66 1.71
ObesityDataSet 4 Centralized 0.13 283.36 2.13 Federated 0.16 349.53 2.08
ObesityDataSet 5 Centralized 0.17 327.37 1.94 Federated 0.25 467.40 1.75
heart disease 2 Centralized 0.17 63.26 2.11 Federated 0.19 68.36 2.03
heart disease 3 Centralized 0.19 55.59 1.87 Federated 0.20 62.43 1.93
heart disease 4 Centralized 0.17 182.40 2.01 Federated 0.43 123.97 1.32
heart disease 5 Centralized 0.45 121.40 1.20 Federated 0.63 209.60 0.96
custom 2 Centralized 0.59 726.53 0.63 Federated 0.60 731.56 0.62
custom 3 Centralized 0.76 2992.18 0.35 Federated 0.56 1748.00 0.80
custom 4 Centralized 0.59 2343.33 0.84 Federated 0.66 2597.46 0.73
custom 5 Centralized 0.56 2344.11 0.78 Federated 0.68 2936.42 0.77
Breast Cancer 2 Centralized 0.34 267.69 1.32 Federated 0.30 260.51 1.33
Breast Cancer 3 Centralized 0.30 208.42 1.41 Federated 0.29 219.32 1.44
Breast Cancer 4 Centralized 0.32 212.07 1.20 Federated 0.32 220.81 1.29
Breast Cancer 5 Centralized 0.41 268.48 0.99 Federated 0.52 354.95 1.01
4.1 Performance Analysis
Tables 2, 3, and 4 provide an overview of the per-
formance achieved with the centralized and federated
approaches across three data distribution scenarios.
Each row represents a separate run with different set-
tings in terms of dataset and number of clusters, so
each run was evaluated with both centralized and fed-
erated approaches. We consider here, as clustering-
quality indexes, the Calinski-Harabasz (CH), the Sil-
houette, and the Davies-Bouldin ones, respectively.
CH provides information on how well-separated and
compact the clusters are. The lower the CH, the better.
The silhouette index summarizes clusters’ cohesion
(proximity of points inside the same cluster) and sep-
aration (distance between clusters). Its values range
between -1 and 1, where -1 indicates a misclassifi-
cation. The higher the value, the better. Finally, the
Davies-Bouldin (DB) index tells us how similar the
clusters are, with intra-cluster dispersion and inter-
cluster separation. In this case, the lower the value,
the better. Focusing on hard-heterogeneous data dis-
tribution (Table 2), we notice an improvement of all
the indices while considering the federated clustering
method against the clustering performed classically.
The improvement is still evident for data soft distri-
bution (Table 4) and less noticeable for heterogeneous
data distribution (Table 3).
The data reported in the tables represent averages
calculated from multiple training runs. Performance
was evaluated using three metrics: 1) the Silhouette
score utilized to assess the cohesion and separation of
clusters; it ranges from -1 to 1, with higher scores in-
dicating better clustering performance. 2) the Davies-
Bouldin index (DBI) that measures the ratio of within-
cluster distances to between-cluster distances; a lower
score indicates better clustering quality, and 3) the
Calinski-Harabasz index (CHI) evaluates the ratio of
between-cluster dispersion to within-cluster disper-
sion; a higher score indicates better-defined clusters.
From a high-level analysis, the results clearly
show that the centralized approach does not consis-
tently outperform the federated approach; on the con-
trary, federated approaches are proving to be highly
competitive. Looking at the results in Table 2 for the
hard distribution scenario, it is noticeable that feder-
ated approaches outperform centralized approaches in
14 out of 20 reported runs. Here, ’outperform’ means
that federated approaches give better results in at least
2 out of 3 metrics.
For H and SH scenarios (see tables 3 and 4), cen-
tralized approaches are more effective in 11 out of 20
runs and 13 out of 20 runs, respectively.
To further support the competitiveness of the ap-
proach, the average performance gap between the
centralized and federated approaches is generally
modest across all scenarios. Here, the gap is cal-
culated as the average difference between the corre-
sponding pairs of metrics for each run, considering
NCTA 2024 - 16th International Conference on Neural Computation Theory and Applications
554
Table 3: Overview of the Performance Results - Homogeneous Distribution.
Dataset Clusters Approach Silhouette
Calinski
Harabasz
Davies
Bouldin
Approach Silhouette
Calinski
Harabasz
Davies
Bouldin
oasis2 2 Centralized 0.19 76.40 2.00 Federated 0.19 76.12 1.99
oasis2 3 Centralized 0.18 74.28 1.78 Federated 0.18 74.21 1.78
oasis2 4 Centralized 0.18 67.19 1.64 Federated 0.17 65.48 1.73
oasis2 5 Centralized 0.15 60.67 1.69 Federated 0.15 58.98 1.76
ObesityDataSet 2 Centralized 0.19 277.98 2.53 Federated 0.10 201.84 2.94
ObesityDataSet 3 Centralized 0.14 244.42 2.32 Federated 0.16 163.43 2.28
ObesityDataSet 4 Centralized 0.15 226.26 2.11 Federated 0.14 180.76 1.90
ObesityDataSet 5 Centralized 0.13 222.67 1.96 Federated 0.15 141.32 2.12
heart disease 2 Centralized 0.17 63.26 2.11 Federated 0.17 63.22 2.1
heart disease 3 Centralized 0.14 47.53 2.11 Federated 0.13 47.28 2.22
heart disease 4 Centralized 0.14 43.60 2.04 Federated 0.13 41.07 2.14
heart disease 5 Centralized 0.12 38.28 2.07 Federated 0.13 37.98 2.05
custom 2 Centralized 0.59 726.53 0.63 Federated 0.52 485.43 0.79
custom 3 Centralized 0.75 2918.89 0.36 Federated 0.67 2408.70 0.66
custom 4 Centralized 0.53 2048.49 1.39 Federated 0.54 2043.10 1.38
custom 5 Centralized 0.34 1618.97 1.95 Federated 0.45 1599.02 1.64
Breast Cancer 2 Centralized 0.34 267.69 1.32 Federated 0.35 267.44 1.30
Breast Cancer 3 Centralized 0.31 197.11 1.53 Federated 0.31 196.93 1.53
Breast Cancer 4 Centralized 0.27 158.68 1.51 Federated 0.20 156.09 1.76
Breast Cancer 5 Centralized 0.16 140.16 1.76 Federated 0.16 137.99 1.81
Table 4: Overview of the Performance Results - Soft Distribution.
Dataset Clusters Approach Silhouette
Calinski
Harabasz
Davies
Bouldin
Approach Silhouette
Calinski
Harabasz
Davies
Bouldin
oasis2 2 Centralized 0.19 76.40 2.00 Federated 0.19 76.37 2.00
oasis2 3 Centralized 0.18 74.28 1.78 Federated 0.19 74.22 1.77
oasis2 4 Centralized 0.18 67.19 1.64 Federated 0.17 65.00 1.70
oasis2 5 Centralized 0.15 60.67 1.69 Federated 0.16 59.16 1.72
ObesityDataSet 2 Centralized 0.19 277.98 2.53 Federated 0.19 277.76 2.53
ObesityDataSet 3 Centralized 0.14 244.42 2.32 Federated 0.15 228.32 2.33
ObesityDataSet 4 Centralized 0.1 5 226.26 2.11 Federated 0.12 223.13 2.21
ObesityDataSet 5 Centralized 0.13 222.67 1.96 Federated 0.15 213.95 2.07
heart disease 2 Centralized 0.17 63.26 2.11 Federated 0.17 63.24 2.11
heart disease 3 Centralized 0.14 47.53 2.11 Federated 0.14 47.18 2.25
heart disease 4 Centralized 0.14 43.60 2.04 Federated 0.14 42.63 2.04
heart disease 5 Centralized 0.12 38.28 2.07 Federated 0.13 38.35 2.03
custom 2 Centralized 0.59 726.53 0.63 Federated 0.56 625.57 0.69
custom 3 Centralized 0.75 2918.89 0.36 Federated 0.75 2918.89 0.36
custom 4 Centralized 0.53 2048.49 1.39 Federated 0.50 1597.72 1.45
custom 5 Centralized 0.34 1618.97 1.95 Federated 0.48 1594.48 1.54
Breast Cancer 2 Centralized 0.34 267.69 1.32 Federated 0.34 267.65 1.31
Breast Cancer 3 Centralized 0.31 197.11 1.53 Federated 0.32 196.47 1.54
Breast Cancer 4 Centralized 0.27 158.68 1.51 Federated 0.19 156.15 1.79
Breast Cancer 5 Centralized 0.16 140.16 1.76 Federated 0.16 137.18 1.79
all runs performed for each scenario. In fact, in Ta-
ble 5, it is noticeable that the average gaps are small.
For example, in the SH scenario, the average gap for
the Silhouette is 0, indicating that even when the cen-
tralized approach performs better, the difference from
the federated approach is minimal. From Table 5, we
observe that, in the homogeneous case, the silhou-
ette worst gap is circa 0, that is, the point is close to
the decision boundary between the considered clus-
ters. Moving from the homogeneous data distribution
to the soft heterogeneous one, the silhouette worst
gap is equal to 0 and slightly below 0 for the hard-
A Federated K-Means-Based Approach in eHealth Domains with Heterogeneous Data Distributions
555
Table 5: Performance Gap Between Data Distribution Scenario.
Data
Distribution
Silhouette
Average Gap
Calinski-Harabasz
Average Gap
Davies-Bouldin
Average Gap
Silhouette
Worst Gap
Calinski-Harabasz
Worst Gap
Davies-Bouldin
Worst Gap
Homogeneous 0.0085 53.63 -0.053 0.08 0.30 -2.58
Hard Heterogeneous -0.04 -10.68 0.02 0.08 -6.84 -2.56
Soft Heterogeneous 0 30.78 -0.02 0 -0.06 -2.17
Table 6: Cluster similarity analysis.
ARI FMI
Alzheimer’s Disease
H-scenario 0.95 0.98
SH-scenario 1 1
HH-scenario 0.91 0.96
Heart Disease
H-scenario 0.93 0.96
SH-scenario 1 1
HH-scenario 0.88 0.94
Obesity
H-scenario 0.1 0.58
SH-scenario 0.96 0.98
HH-scenario 0.72 0.86
Breast Cancer
H-scenario 0.94 0.97
SH-scenario 1 1
HH-scenario 0.94 0.97
Custom
H-scenario 1 1
SH-scenario 1 1
HH-scenario 1 1
heterogeneous case, thus showing a certain stability
with respect to the passage toward the inhomogene-
ity. A higher instability is shown by the average gap in
the Calinski-Harabasz index, from soft to hard homo-
geneous. Finally, the Davies-Bouldin index presents
only a small clustering-quality diminution concerning
the worst gap, even between homogeneous and hard-
heterogeneous data distribution. It’s also interesting
to note that the average gap value for the Calinski-
Harabasz metric ranges from -0.053 to 0.02, indicat-
ing that the clusters are well separated with low intra-
cluster variance and high inter-cluster variance.
In addition, Table 5 also reports the gap between
the worst-performing runs among all runs for each
data distribution. Even in these cases, the gaps for
the Silhouette and Calinski-Harabasz metrics remain
small. However, the Davies-Bouldin gap is larger
than the average gap.
These results aim to demonstrate the effectiveness
of the proposed approach by comparing it with tra-
Table 7: Clusters composition of Alzheimer’s patients ob-
tained with the Centralised approach. EDUC- Education
level; SES - Socio-Economic Status; eTIV - estimated To-
tal Intracranial Volume; Normalized Whole Brain Volume
- nWBV; MMSE - Mini-Mental State Examination; CDR -
Clinical Dementia Rating.
Cluster 1 Cluster 2
Age
Mean (Std) 76.29 ± 7.3 77.46± 8.0
Range [61, 98] [60, 97]
Sex
Female # (%) 51 (39.53%) 153 (68%)
Male # (%) 78 (60.47%) 72 (32%)
EDUC (years)
Mean (Std) 13.79 ± 3.01 15.23 ± 2.69
Range [6, 20] [8, 23]
SES
Mean (Std) 2.79 ± 1.19 2.27 ± 1.05
Range [1, 5] [ 1, 5]
eTIV
Mean (Std) 1494.34 ± 172.84 1487.5 ± 176.99
Range [1143.0, 1957.0] [1106.0, 2004.0]
nWBV
Mean (Std) 0.71 ± 0.03 0.74 ± 0.04
Range [0.65, 0.81] [0.64, 0.84]
MMSE
Mean (Std) 24.39 ± 4.63 ) 29.14 ( 1.04 )
Range [4, 30] [24, 30]
CDR
Mean (Std) 0.67 ±0.31 0.04 ± 0.14
Range [ 0, 2] [0, 0.5]
Diagnosis
CN 2 (1.6%) 188 (83.6%)
AD 127 (98.4%) 0 (0%)
Converted 0 (0%) 37 (16.4%)
ditional centralized K-means. The performance from
a more general perspective provides insight into the
results in terms of the evaluation metrics. Thus, the
evaluation of the average and worst gaps highlights
the approach’s consistency, showing that even in aver-
age and worst-case scenarios, the proposed federated
approach converges to the centralized one.
4.2 Similarity Clusters Analysis
To determine the quality of the cluster composition
generated by the federated approach, we compare the
similarity between the clusters identified by the cen-
NCTA 2024 - 16th International Conference on Neural Computation Theory and Applications
556

Table 8: Clusters of AD patients obtained with the federated
approach under homogeneous distribution settings.
Cluster 1 Cluster 2
Age
Mean (Std) 76.53 ± 7.21 77.31 ± 89
Range [61, 98] [60, 97]
Sex
Female # (%) 49 (39.2%) 155 (67.69%)
Male # (%) 76 (60.8) % 74 (32.31%)
EDUC
Mean (Std) 13.69 ± 2.99 15.26 ± 2.68
Range [6, 20] [8, 23]
SES
Mean (Std) 2.85 ± 1.17 2.25 ± 15
Range [1, 5] [1, 5]
eTIV
Mean (Std) 1492.74 ± 170 1488.49 ± 178.44
Range [1143 1957] [1106 2004]
nWBV
Mean (Std) 0.71 ± 03 0.74 ± 04
Range [0.65, 0.81] [0.64, 0.84]
MMSE
Mean (Std) 24.25 ± 4.63 29.14 ± 14
Range [4, 30] [24, 30]
CDR
Mean ± Std 0.67 ± 0.31 05 ± 0.15
Range [0, 2] [0, 0.5]
Diagnosis
CN 2 (1.6%) 188 (82.1%)
AD 123 (98.4%) 4 (1.7%)
Converted 0 (0%) 37 (16.2%)
tralized approach and those identified by the feder-
ated one using two similarity measures: 1) Adjusted
Rand Index (ARI), while Rand Index (RI) measures
cluster similarity through the percentage of consistent
decisions between two clustering, the Adjusted Rand
Index (ARI) corrects the RI by the chance grouping
of elements, providing more robust statistics for com-
paring different clustering algorithms or methods; 2)
Fowlkes–Mallows index (FMI) is a metric used to
evaluate the clusters similarity obtained through vari-
ous clustering algorithms. It is typically used to evalu-
ate the clustering performance of a specific algorithm
by assuming that the obtained cluster is compared to
the ground truth–i.e., the perfect cluster.
To adopt such indexes, we assume that the results
of the centralised clustering approach are the bench-
mark clusters to be compared.
The indexes obtained from the comparison be-
tween the centralised approach and the federated
approach in three different scenarios and for each
dataset are presented in Table 6. It can be noted that
significant heterogeneity within the data may result
in diminished cluster composition quality in feder-
ated k-means, analogously to the case of traditional
supervised federated-learning methodologies. Never-
Table 9: Clusters of AD patients obtained with the federated
approach under soft distribution settings.
Cluster 1 Cluster 2
Age
Mean (Std) 76.29 ± 7.3 77.46± 8.0
Range [61, 98] [60, 97]
Sex
Female # (%) 51 (39.53%) 153 (68%)
Male # (%) 78 (60.47%) 72 (32%)
EDUC
Mean (Std) 13.79 ± 3.01 15.23 ± 2.69
Range [6, 20] [8, 23]
SES
Mean (Std) 2.79 ± 1.19 ) 2.27 ± 1.05
Range [1, 5] [ 1, 5]
eTIV
Mean (Std) 1494.34 ± 172.84 1487.5 ± 176.99
Range [1143.0, 1957.0] [1106.0, 2004.0]
nWBV
Mean (Std) 0.71 ± 0.03 0.74 ± 0.04
Range [0.65, 0.81] [0.64, 0.84]
MMSE
Mean (Std) 24.39 ± 4.63 ) 29.14 ( 1.04 )
Range [4, 30] [24, 30]
CDR
Mean (Std) 0.67 ±0.31 0.04 ± 0.14
Range [ 0, 2] [0, 0.5]
Diagnosis
CN 2 (1.6%) 188 (83.6%)
AD 127 (98.4%) 0 (0 %)
Converted 0 (0%) 37 (16.4%)
theless, a noteworthy outcome indicates that soft het-
erogeneity provides advantages in federated settings.
This specific finding manifests with greater promi-
nence in the Obesity dataset, which encompasses a
fourfold greater number of samples than the Breast
Cancer and Custom datasets, six times more than the
Oasis2 and Heart Disease datasets. Indeed, the anal-
ysis reveals that the ARI for the Obesity dataset dis-
plays a notably low performance in the homogeneous
scenario. At the same time, there is a notable increase
in the SH scenario and a somewhat lesser increase in
the HH scenario.
Finally, to further demonstrate the efficacy of the
federated approach in generating comparative out-
comes with the classical centralized K-means method,
we present a descriptive analysis of the clusters iden-
tified through both approaches across three speci-
fied scenarios using the OASIS2 dataset related to
Alzheimer’s disease. Such a dataset was selected
based on its unique provision of patients’ diagnoses,
which allows for a more practical demonstration of
similarities and differences among clusters compared
to other available datasets.
The clusters resulting from the centralized K-
means approach and the federated one with homoge-
A Federated K-Means-Based Approach in eHealth Domains with Heterogeneous Data Distributions
557

Table 10: Clusters of AD patients using the federated ap-
proach under Hard Heterogeneous distribution settings.
Cluster 1 Cluster 2
Age
Mean (Std) 76.94 ± 8.34 79.26 ± 8.21
Range [ 66.0 , 98.0 ] [ 60.0 , 97.0 ]
Sex
Female # (%) 45 ( 40.18 %) 161 ( 66.53 %)
Male # (%) 67 ( 59.82 %) 81 ( 33.47 %)
EDUC
Mean (Std) 13.16 ± 3.14 15.1 ± 2.76
Range [ 6.0 , 20.0 ] [ 8.0 , 23.0 ]
SES
Mean (Std) 2.96 ± 1.16 2.34 ± 1.09
Range [ 1.0 , 5.0 ] [ 1.0 , 5.0 ]
eTIV
Mean ± SD 1465.46 ± 154.55 1489.93 ± 199.58
Range [ 1143.0 , 1911.0 ] [ 1154.0 , 2004.0 ]
nWBV
Mean (Std) 0.71 ± 0.04 0.73 ± 0.04
Range [ 0.65 , 0.81 ] [ 0.66 , 0.84 ]
MMSE
Mean (Std) 23.04 ± 5.18 28.95 ± 1.17
Range [ 4.0 , 30.0 ] [ 24.0 , 30.0 ]
CDR
Mean (Std) 0.67 ± 0.29 0.06 ± 0.16
Range [ 0.5 , 2.0 ] [ 0.0 , 0.5 ]
Diagnosis
CN 0 (0%) 201 (83.1%)
AD 112 (100%) 3 (1.2%)
Converted 0 (0%) 38 (15.7%)
neous data distribution are shown in Tables 7 and 8.
The clusters identified by the proposed feder-
ated K-means closely resemble those identified by
the classical K-means, as evidenced by the indexes
presented in Table 6. The federated K-means al-
gorithm successfully clustered 123 individuals with
Alzheimer’s disease, while the classical K-means al-
gorithm clustered 127 individuals with the same con-
dition. Both methods categorized an equal number of
cognitively normal subjects and subjects likely to ex-
perience a conversion into cluster #2.
Moreover, Tables 9 and 10 show the clusters
detected by the federated approach under hetero-
geneous data distribution, Soft-Heterogeneous and
Hard-Heterogeneous distribution, respectively. As
observed, in cases of a soft distribution condition, the
federated approach demonstrates performance com-
parable to that of the traditional K-means algorithm.
Any slight discrepancies identified in the preceding
condition are mitigated, as evidenced by the indexes
presented in Table 6. On the contrary, when the data
distribution is heavily unbalanced under the previous
conditions, the discriminatory power of the federated
K-means decreases.
5 CONCLUSIONS
Federated Learning (FL) represents an emerging trend
in machine learning. This approach allows for the de-
velopment of a global model without sharing private
data distributed among multiple data owners. Signifi-
cant research in the field of FL has primarily focused
on applying supervised learning techniques. On the
contrary, the available literature about federated un-
supervised learning is still limited.
In particular, among unsupervised techniques,
clustering has shown numerous beneficial applica-
tions in the healthcare domain. Hence, the advance-
ment of federated clustering has the potential to ad-
dress certain limitations associated with data usage,
particularly privacy concerns, which currently hinder
the full realization of the vast potential of health data-
clustering approaches. Moreover, the performance
of Federated Learning is found to be satisfactory in
scenarios where data are independent and identically
distributed (IID). Conversely, in cases where data
are non-independent and non-identically distributed
(Non-IID), it becomes challenging to effectively train
a machine learning algorithm that relies on global
measures while ensuring that all data remain local.
The current study presents a new federated K-
means clustering framework based on a global cosine-
similarity measure to enhance the trade-off between
privacy preservation and clustering effectiveness.
Furthermore, our investigation explores the impact of
the heterogeneous health data-distribution hypothesis
on the convergence of both local and global models.
The efficacy of the proposed federated K-means
algorithm has been evaluated across diverse health-
care datasets and under various experimental condi-
tions, with a comparative analysis of its performance
against the centralized K-means algorithm. Accord-
ing to the initial results, while dealing with hetero-
geneous distributions of health data, the difference
between the centralized and federated approaches is
minimal, and the federated approach demonstrates
promising potential. The decentralized approach ex-
hibits superior performance when evaluated on cer-
tain healthcare datasets compared to the centralised
one. Finally, the results of this study provide empiri-
cal evidence that diversity within federated networks
can have a beneficial effect on the overall quality of
cluster composition.
Future developments of this research can also ad-
dress the challenges associated with heterogeneous
data distributions in federated learning, for instance,
divergence of local models, and slow or unstable con-
vergence, or class imbalance. The detailed explo-
ration of solutions to undertake in these cases can
NCTA 2024 - 16th International Conference on Neural Computation Theory and Applications
558

strengthen the proposed clustering approach.
Future work will focus on evaluating the approach
on larger datasets while removing the assumption of
equal probability-distributions among clients.
ACKNOWLEDGEMENTS
This paper was developed within the project funded
by Next Generation EU - “Age-It - Ageing well in
an ageing society” project (PE0000015), National Re-
covery and Resilience Plan (NRRP) - PE8 - Mission
4, C2, Intervention 1.3. The views and opinions ex-
pressed are only of the authors and do not necessarily
reflect those of the European Union or the European
Commission.
REFERENCES
Abid Ali Awan (2021). Heart Disease patients -
Targeting treatment for heart disease patients.
URL: https://www.kaggle.com/datasets/kingabzpro/
heart-disease-patients.
Act, A. (1996). Health insurance portability and account-
ability act of 1996. Public law, 104:191.
Battineni, G., Chintalapudi, N., and Amenta, F. (2019).
Data for: Machine learning in medicine: performance
calculation of dementia prediction by support vector
machines (SVM). Mendeley Data.
Bharati, S., Mondal, M. R. H., Podder, P., and Prasath, V. S.
(2022). Federated learning: Applications, challenges
and future directions.
Bonawitz, K., Kairouz, P., McMahan, B., and Ramage,
D. R. (2021). Federated learning and privacy. ACM
Queue, 19.
Brand
˜
ao, A., Mendes, R., and Vilela, J. P. (2021). Ef-
ficient Privacy Preserving Distributed K-Means for
Non-IID Data. In Abreu, P. E., Pereira Rodrigues, P.,
Fern
´
andez, A., and Gama, J., editors, Advances in In-
telligent Data Analysis XIX, 19th International Sym-
posium on Intelligent Data Analysis, IDA 2021, vol-
ume 12695, pages 439–451. Springer.
Dhade, P. and Shirke, P. (2024). Federated learning for
healthcare: A comprehensive review. Engineering
Proceedings, 59(1):230.
Garst, S. and Reinders, M. (2024). Federated K-Means
Clustering. ArXiV preprint, arXiv:2310.01195v2.
Liu, Y., Ma, Z., Yan, Z., Wang, Z., Liu, X., and a, J. (2020).
Privacy-preserving federated k-means for proactive
caching in next generation cellular networks. Infor-
mation Sciences, 521:14–31.
Marulli, F., Balzanella, A., Campanile, L., Iacono, M., and
Mastroianni, M. (2021a). Exploring a federated learn-
ing approach to enhance authorship attribution of mis-
leading information from heterogeneous sources. In
2021 International Joint Conference on Neural Net-
works (IJCNN), pages 1–8.
Marulli, F., Verde, L., Marrone, S., Barone, R., and De Bi-
ase, M. S. (2021b). Evaluating efficiency and effec-
tiveness of federated learning approaches in knowl-
edge extraction tasks. In 2021 International Joint
Conference on Neural Networks (IJCNN), pages 1–6.
Palechor, F. M. and De la Hoz Manotas, A. (2019). Dataset
for estimation of obesity levels based on eating habits
and physical condition in individuals from colombia,
peru and mexico. Data in brief, 25:104344.
Pedrycz, W. (2022). Federated FCM: Clustering Under Pri-
vacy Requirements. IEEE Transactions on Fuzzy Sys-
tems, 30(8):3384–3388.
Sheller, M. J., Edwards, B., Reina, G. A., Martin, J., Pati,
S., Kotrotsou, A., Milchenko, M., Xu, W., Marcus,
D., Colen, R. R., et al. (2020). Federated learning
in medicine: facilitating multi-institutional collabora-
tions without sharing patient data. Scientific reports,
10(1):12598.
Stallmann, M. and Wilbik, A. (2022). On a Framework
for Federated Cluster Analysis. Applied Sciences,
12(10455).
Voigt, P. and Von dem Bussche, A. (2017). The eu gen-
eral data protection regulation (gdpr). A Practical
Guide, 1st Ed., Cham: Springer International Pub-
lishing, 10(3152676):10–5555.
W. H. Wolberg, W. N. S. and Mangasarian, O. L.
(2017). Breast cancer Wisconsin (diagnos-
tic) data set. URL: https://www.kaggle.com/
datasets/nancyalaswad90/breast-cancer-dataset.
Wahab, O. A., Mourad, A., Otrok, H., and Taleb, T. (2021).
Federated machine learning: Survey, multi-level clas-
sification, desirable criteria and future directions in
communication and networking systems. IEEE Com-
munications Surveys Tutorials, 23(2):1342–1397.
Yang, K., Mohammadi Amiri, M., and Kulkarni, S. R.
(2024). Greedy centroid initialization for federated K
-means. Knowledge and Information Systems.
Zhu, S., Xu, Q., Zeng, J., Wang, S., Sun, Y., Yang, Z., and
Oeng, Z. (2023). F
3
KM: Federated, Fair, and Fast k-
means. Proc. ACM Manag. Data, 1(4):241.
A Federated K-Means-Based Approach in eHealth Domains with Heterogeneous Data Distributions
559
