
System DietadHoc: A Fusion of Human-Centered Design and Agile
Development for the Explainability of AI Techniques Based on
Clinical and Nutritional Data
Michelangelo Sofo
1,* a
, Giuseppe Labianca
2,* b
, Giancarlo Mauri
3,* c
and
Francesco Combierati
4,* d
1
IT Consultant, Via Avvocato Vittorio Malcangi, 141/L, 76125, Trani, Italy
2
Dietician and Nutritionist Biologist, Via Tenente Morrico, 17, 76125, Trani, Italy
3
University of Milano – Bicocca, Piazza dell’Ateneo Nuovo, 1, 20126, Milano, Italy
4
Dipartimento di Scienze Economiche, Piazza Scaravilli, 2, 40126, Bologna, Italy
Keywords: Medical Decision Support System, Physiological Data Extraction, Human Centered Design (HCD), Contextual
Design, Participatory Design, Rapid Prototyping, Agile Development, Continuous Optimization Algorithms,
Human Centered Artificial Intelligence (HCAI), Time Series Analysis, Visual Data Mining, Deductive Database.
Abstract: In recent years, the scientific community's interest in the exploratory analysis of biomedical data has increased
exponentially. Considering the field of research of nutritional biologists, the curative process, based on the
analysis of clinical data, is a very delicate operation due to the fact that there are multiple solutions for the
management of pathologies in the food sector (for example can recall intolerances and allergies, management of
cholesterol metabolism, diabetic pathologies, arterial hypertension, up to obesity and breathing and sleep
problems). In this regard, in this research work a system was created capable of evaluating various dietary
regimes for the aforementioned specific patient pathologies. The system is based on a mathematical-numerical
model and is tailored for the real working needs of experts in human nutrition, endocrinologists and cardiologists,
using the Human-Centered Design (HCD - ISO 9241 210). DietAdhoc is a decision support system to the
aforementioned specialists for patients of both sexes (from 18 years of age) developed with an innovative agile
methodology. The software consists in drawing up the biomedical and clinical profile of the specific patient by
applying two implementation approaches on nutritional data.
1 INTRODUCTION
Food science is currently an area of particular
scientist interest, both for software developers, and
for the clinical specialists involved (nutritional
biologist, cardiologists, diabetologists and
endocrinologists). "Do it yourself" diet software,
advertised on internet, television and in newspapers,
are often followed by people with various types of
nutritional problems. In this research work the direct
a
https://orcid.org/0009-0004-7928-1331
b
https://orcid.org/0009-0009-3971-5218
c
https://orcid.org/0000-0003-3520-4022
d
https://orcid.org/0000-0002-6832-8147
* These authors contributed equally.
1
dietup.it
2
easydiet.it
interaction with a dietician - nutritional biologist made
it possible to highlight that the problem with such lies
in the fact that, once tested, they generate approximate
and incomplete results, often causing situations of
malnutrition. Basing on the HCD approach, in the user
– research phase (Mastrangelo et al., 2015), and under
the supervision of the nutritional biologist involved in
the creation of the DietAdhoc system, twelve
commercial software tools (DietUp
1
, Easy Diet
2
,
Sofo, M., Labianca, G., Mauri, G. and Combierati, F.
System DietadHoc: A Fusion of Human-Centered Design and Agile Development for the Explainability of AI Techniques Based on Clinical and Nutritional Data.
DOI: 10.5220/0013054800003911
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 18th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2025) - Volume 1, pages 519-528
ISBN: 978-989-758-731-3; ISSN: 2184-4305
Proceedings Copyright © 2025 by SCITEPRESS – Science and Technology Publications, Lda.
519

Evolution Fit
3
, Fatsecret
4
, Melarossa
5
, MetaDieta
6
,
Myfitnesspal
7
, Nutribook
8
, Nutrium
9
, Nutriverso
10
,
SifaDieta
11
, Winfood
12
) have been evaluated in all
their functionality. It was found that the
aforementioned software tools, available through
various subscription formulas, present generic and
redundant functions and therefore are incomplete for
all the clinical. Practically such systems don’t
adequately support end user (specialists in human
nutrition, cardiologists, diabetologists and
endocrinologists) for their lack of explainability and
reliability. During this assessment, it has been
possible to highlight the absence of an exploratory
analysis of a patient’s clinical and nutritional data and
a poor attention to the relevant aspects, specifically in
the following areas:
• allergies and intolerances (shellfish, dried fruit,
mushrooms, gluten, lactose, yeasts, nickel and
other);
• analysis of the pathological history with
possible familiarity (anemia, autoimmune
pathologies, endocrine pathologies, oncological
pathologies and cardiovascular risk);
• functional anamnesis analysis (abdominal pain,
bowel movements, asthenia, menstrual cycle,
dermatitis, dyspepsia, eczema, hiatal hernia,
stools, smoking, gastritis, abdominal swelling,
loss of appetite and myalgia);
• analysis of sports activity (type of discipline and
daily frequency);
• complete evaluation of total blood chemistry
tests (azotemia, blood urea nitrogen, blood
glucose, creatinine, direct bilirubin, indirect
bilirubin, total bilirubin, total cholesterol,
cardiovascular risk index, chemical test of urine,
cholesterol HDL, cholesterol LDL, creatinine,
eGFR, mGFR, complete blood count, ferritin,
glycolysed hemoglobin (HbA1c), Homa Index
IR, Homa – β, insulinemia, homocysteine,
hormonal dosages, iron level in blood,
triglyceridemia, transaminases GOT,
transaminanes GPT);
• any therapies in progress, or taken in the last few
months (name of the drug with relative dosage);
• section in which the nutritional biologist can
insert complementary clinical notes;
• dynamic configurators for determining the
macronutrients to be consumed daily
3
evolutionfit.it
4
fatsecret.it
5
melarossa.it
6
metadieta.it
7
myfitnesspal.com
(carbohydrates, proteins and fats) for evaluating
the kilocalories and micronutrients (cholesterol,
fibers, potassium, sodium, etc.) to be consumed
in the various meals of the day;
• ORAC values (antioxidant power of foods) to
counteract cellular aging (Haytowitz D.B. et
al.,2010);
• PRAL values (renal acid load potential) to
calculate the chemical balance of the acidifying
and alcalinisant molecules of a food (Remer et
al., 1995);
• BIA data, (obtained from the bioelectric
impedance analysis) – (Mehra et al., 2024);
• glycemic index of a food (Scazzina F. et al.,
2016);
• glycemic load, calculated based on the quantity
of carbohydrates in the food portion in grams for
the specific glycemic index (Scazzina F. et.al.,
2016);
• absence of the glycemic curve of the meal;
• absence of the weight history (current weight,
desirable weight, ideal weight).
These gaps obviously cause an approximation of the
patient's clinical profile. As will be explained in detail
in the following chapters, the objective of this research
word consists in creating a virtuous integration
between the consolidated clinical experience of a
specialist in human nutrition and its supporting
technical equipment to create a software that improve
patient well-being and help prevent diseases (Figure
1).
Figure 1: DietAdhoc’s virtuos integration.
8
nutribook.app
9
nutrium.com
10
nutriverso.cloud
11
sifadieta.com
12
winfood.it
BIOINFORMATICS 2025 - 16th International Conference on Bioinformatics Models, Methods and Algorithms
520

2 DIETADHOC DESIGN
During the user research phase of HCD approach, the
designer of the DietAdhoc system takes into account
various clinical checks and visits carried out by the
nutritional biologist (ethnographic research).
Following this process, the system designer develops
a series of unstructured interviews and specific
questionnaires to define:
• the complete profile of the characteristics of the
nutritional biologist and of the designer –
system administrator who will use the system
[age, gender, type of interaction with the system
(primary or secondary), frequency of use of the
system (daily, in the specific case), level of
computer experience (inexperienced, sufficient,
good, expert), system usage time and technical
support equipment];
• task analysis (both for the nutritional biologist,
and for the designer - system administrator);
• usage scenarios (both for the nutritional
biologist, and for the designer – system
administrator);
• future stakeholders (cardiologists,
diabetologists and endocrinologists), interested
in scientific collaborations to share clinical
information for the creation of a
multidisciplinary team).
In the initial phase, the two figures in charge of
the software will be the nutritional biologist (domain
expert) and the system designer who will also act as
system administrator. The nutritional biologist, is 32
years old and has basic computer skills. He represents
the primary user of the system because he uses it daily
and deals with the insertion and update of all the
patient’s clinical data (including reports from other
specialists), of a new food portions relating to certain
diets into the database, and for the generation of
clinical reports to be sent via e-mail to patients). The
designer – system administrator, is 42 years old, and
has a high level of computer skills. He represents the
secondary user of the system because he is contacted
on the base of the needs of the nutritional biologist.
The system designer remotely checks for any
malfunctions in the workflow and in the interfacing
with the technical instrumentation.
Subsequently the nutritional biologist has
contacted other medical specialists (cardiologists,
diabetologists and endocrinologists) for the creation
of a scientific multidisciplinary team to support the
DietAdhoc® system. The current technical
instrumentation supporting the human nutrition
specialist consists of: SECA 799 digital column scale,
the SECA mBCA 525 digital bioimpedance meter and
the GIMA digital caliper. At the moment the system
administrator is in contact with the commercial and
technical managers of the aforementioned medical
devices to evaluate the possibility of inserting the
DietAdhoc system into them. Finally, based on the
data obtained from unstructured interviews and
questionnaires, also addressed to the aforementioned
clinical specialists, the designer created usage
scenarios, i.e. descriptions in natural language, of how
the application (with all the tasks identified) will be
used by current and potential users in order to verify
all the needs expressed.
2.1 Requirements
It was found that a software to support a professional
in the field of nutrition, compared to classic data
processing applications coded in a procedural manner,
had to manipulate a knowledge of a clinical nature
with an inferential approach and had to allow an
analysis of the patient with three levels of detail:
• descriptive – analyze the data of the various
patients to decipher the latent details that escape
medical procedures;
• predictive – creation of analytical and complete
models from the aforementioned latent data with
the aim of predicting valid results from the
scientific community in the nutritional field;
• prescriptive - suggest corrective clinical actions
for a given patient, using all the information that
the system has generated.
In this regard, the operational knowledge was codified
in the system by the designer and the following high
fidelity prototypes were created (Conceptual design -
second phase of HCD process):
• a section concerning four food categories (main
food, vegetables, fruit and drinks) so that the
nutritional biologist can insert, update and delete
food portions with the relative contribution in
kilocalories (kcal), macronutrients
(carbohydrates, proteins and fats) and other
nutritional parameters (cholesterol, ORAC,
PRAL, and salts);
• a section for all patient data (name, surname, age,
birth of date, gender, identity document, tax id
code, telephone reference, e-mail, working
activity, eventual Vat number);
• a section for entering medical reports of other
professionals;
• a dynamic menu for evaluating the patient's
medical history, blood chemistry tests and
System DietadHoc: A Fusion of Human-Centered Design and Agile Development for the Explainability of AI Techniques Based on Clinical
and Nutritional Data
521
current therapies;
• an accurate generator of anthropometric
parameters based on seven basic measures
from which all the others are derived;
• two menus for evaluating bioelectric
impedance vector analysis (BIVA) and the
analysis with digital caliper;
• two automatic food regime configurators;
• three heuristic algorithms based on clinical
and nutritional data.
In the third phase of HCD process (Evaluation),
the nutrition biologist carries out a thinking aloud
usability test, designed by the system administrator,
to evaluate the prototypes created in the conceptual
design. All the functions can be viewed in the
demonstration session of the system present at this
link:
https://drive.google.com/file/d/1tnHvpCYAw444Oc2
8-mighNLX9SmV_Of-/view?usp=sharing
From the aforementioned demo, it has been found
that the HCD design process is the conceptually
correct model for the creation of decision support
systems for human health professionals; the product
is seen, even partially, from the beginning of the
process and is perfected in subsequent increments. In
this way, the nutritional biologist, continuously
interfacing with the system administrator, can
continually experiment with each implementation
choice, immediately discarding the wrong ones
(Figure 2).
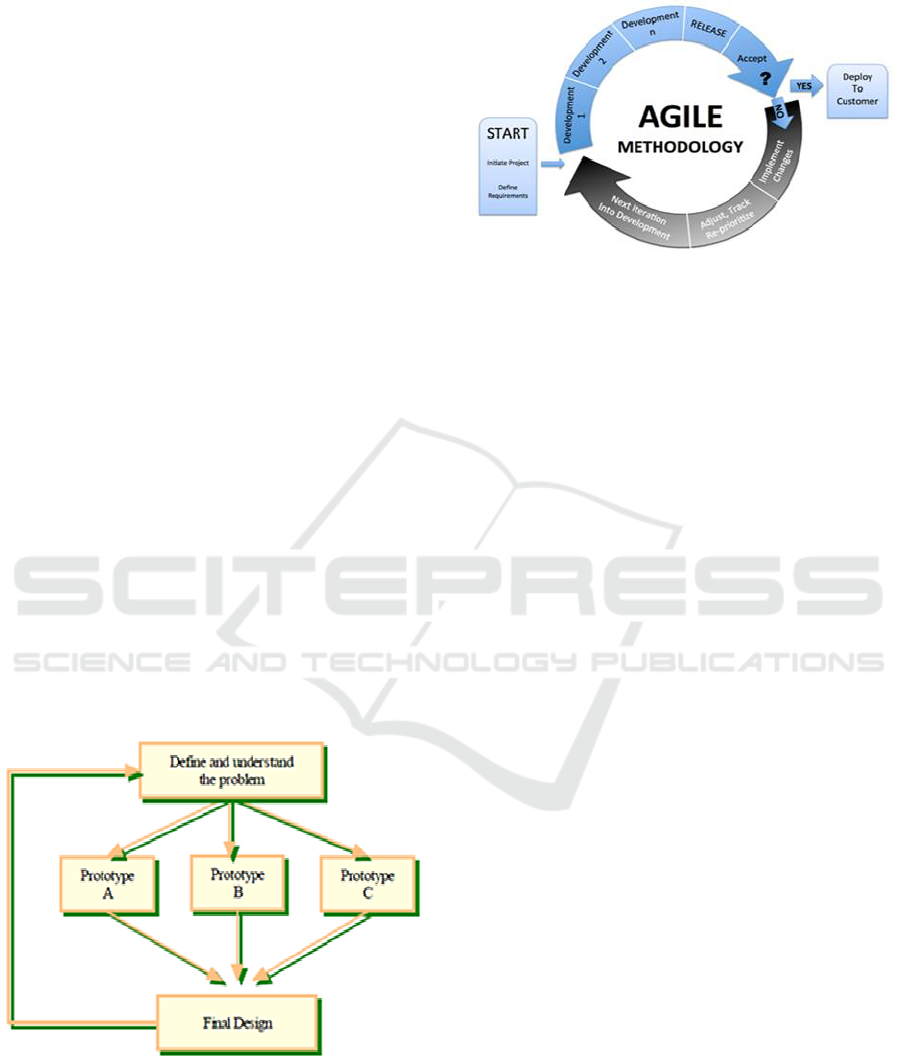
Figure 2: Iterative HCD Design Process adopted for
DietAdhoc System.
Each prototypes of the DietAdhoc® system have
been developed in Java language with an agile
methodology (Figure 3) until the beta version of the
DietAdhoc system is created.
Figure 3: Agile development adopted for DietAdhoc system.
The iterative design, the user involvement, the
continuous prototyping and testing unite HCD Design
process and Agile Development.
3 MATHEMATICAL MODEL
Unlike commercial software in the biomedical-
nutritional field, mentioned in the section 1, the
DietAdhoc system is founded on a mathematical
model which provides scientific evidence and
empirical evidence to this research work. The model
determines an optimal requirement of daily
kilocalories (in kcal), according to certain constraints
on the requirement of macronutrients (carbohydrates,
proteins and fats in grams), micronutrients
(cholesterol, fibers, potassium, sodium, etc.) and other
nutritional parameters (ORAC, PRAL, glycemic
loads, and salts) basing on patient’s clinical situation.
The specific dietary regime is automated by the
system DietAdhoc which supports the professional in
reaching the final diagnosis through a process of
successive steps with the intervention of the doctor (as
supervision). This model is based on a problem of
continue optimization, therefore the decisional
variables (the kilocalories of each portion of food
belonging to four food categories) are defined on R
n
(continue values). The scope of the study consists to
maximize a quantity (the daily kilocalories for the
specific diet, given by the sum of each combination of
four portions of food, or of n portions chosen through
the next two algorithms) through a function f: R
n
→ R
with S ⊆ R
n
according to the notation max{f(x): x ∈
S}. The function f(x) is a function of n real values
f(x
1
,x
2
,…,x
n
), called objective function, and the set S,
the admissible set, i.e. the set of possible solutions to
the problem. The set S is a subset of ℝ
n
, so x =
(x
1
,x
2
,…, x
n
)
T
is an n-dimensional vector variable.
Every x ∈ S is an admissible solution. The admissible
BIOINFORMATICS 2025 - 16th International Conference on Bioinformatics Models, Methods and Algorithms
522
set S is described by a finite set of inequalities, or
equations, of the type g(x) ≥ b, g(x) = b, g(x) ≤ b
where g being a real-valued function defined on ℝ
n
,
while b ∈ ℝ. More formally, assigned m functions g
i
:
ℝ
n
→ ℝ, i = 1,2…, m. and m real scalars b
i
, we have
that S is expressed in the form: S = {x ∈ ℝ
n
| g
i
(x) ≥
b
i
, i =1,2,…m}. All of that inequalities g
i
(x) ≥ b
i
represents a constraint, (the daily grams of nutrients
to be consumed for the specific diet) and the
admissible set is therefore formed by all those points
x which are solutions of the system of inequalities.
More specifically the objective function f(x) and all
the functions that define the constraints g
i
(x), i =
1,2…,m. are linear, that is expressible in the form
c
1
x
1
+c
2
x
2
+…+c
n
x
n
(Figure 4) where we may take the
costs ci to be equal to unity (c=1) since in a clinical
treatment it is not important to consider the economic
side of food portion.
Formally, by introducing c ∈ ℝ
n
(cost vector),
defined as c = (c
1
,…, c
n
)
T
, x ∈ ℝ
n
, and x = (x
1
,…,x
n
)
T
,
the objective function can be written in vector
notation as:
Figure 4: Objective function.
The decision problem consists in determining the
portions (in kcal) of each portions of food, x
j
, j =
1,2…,n, for the particular diet to be followed, so that
the quantity of the j-th nutrient, present in a portion of
food, is greater than, or equal to, the recommended
value bi, daily requirement (in grams) of the j-th
nutrient.
4 SYSTEM DESCRIPTION
In the specific clinical case, after entering of all the
patient’s clinical data and with the automatic
generation phase of anthropometric values (phases
that can be viewed in the demonstration session of
software in section 2.1), the nutritionist biologist will
evaluate a first dietary regime for the particular diet.
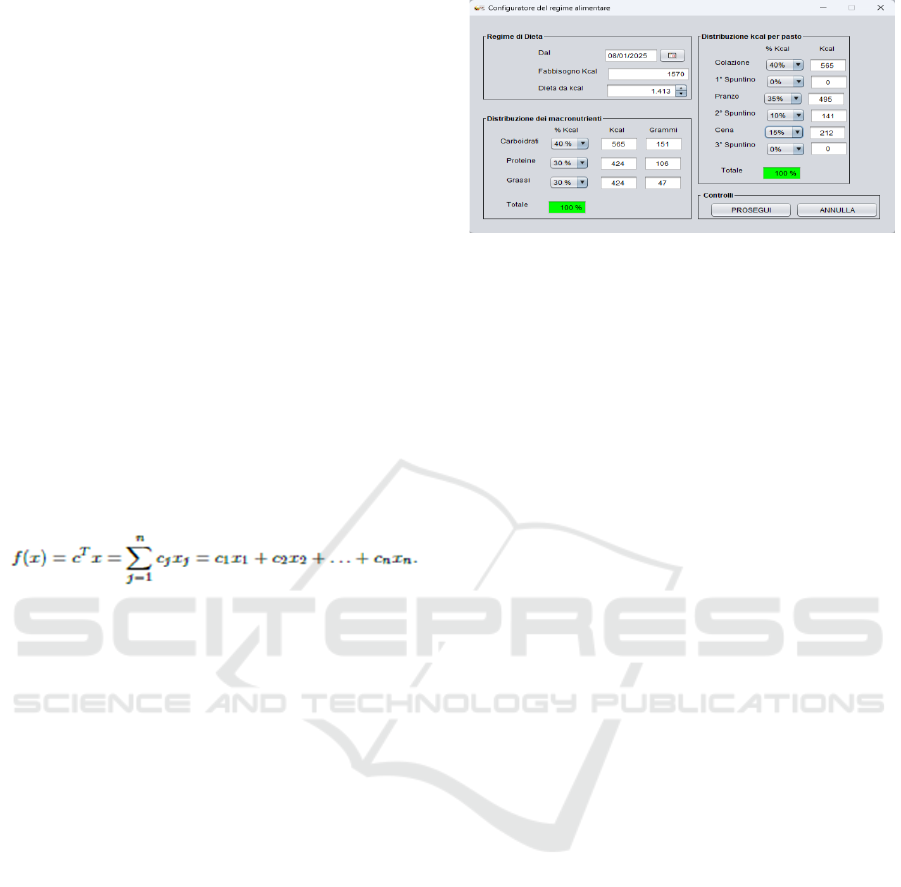
The nutritionist biologist can set the dynamic
configurator that determines the kilocalories of the
diet (1413 – the objective function distributed for four
meals of the day) and the quantity in kilocalories, and
in grams, of macronutrients to be consumed.
Figure 5: Diet configurator.
Two computational approaches have been applied
to process the clinical and nutritional data generated
by the system. The first approach, based on the
enumerative - heuristic algorithm with constraints,
has been designed according to three levels of
abstraction:
• planning of the specific meal which
corresponds to the choice of a combination
made up of four portions of foods belonging to
the categories (main food, vegetables, fruit and
drinks), to be taken within the specific meal
(breakfast, morning snack, lunch, afternoon
snack , dinner and third snack);
• planning of the day which corresponds to the
choice of combinations made up of four
portions of foods to be eaten over the course of
a day (breakfast, morning snack, lunch,
afternoon snack, dinner, and evening snack);
• planning of the week which corresponds to the
choice of the daily combinations made up of
portions of four foods to be consumed over the
course of a week.
This algorithmic approach is based on the first
specialist's modus operandi and considers a
decomposition of the original problem into simpler
sub-problems to solve. It is an implicit enumerative
procedure in several steps. Initially it generates all the
possible solutions (combination of four portions of
food in the research space), then in the next steps the
specialist evaluates the heuristic (“MEDIA
CHILOCALORIE”) and sets the bounds to choose
the optimal food combination of four meals for the
specific patient based on his specific eating disorder.
Naturally, for the specific nutritional problem, the
operating logic of the step of choosing the optimal
food combination is controlled by the nutritional
biologist and is extended for the six meals of the day.
From a conceptual point of view, the technique
implemented in the system for the first enumerative -
System DietadHoc: A Fusion of Human-Centered Design and Agile Development for the Explainability of AI Techniques Based on Clinical
and Nutritional Data
523
heuristic algorithm adopts the following steps:
1. Automatic generation of the n-ary tree of the all set
of eligible solutions S (combination of four portions
of food in the research space) based on the value of
the objective function (kilocalories for the specific
meal – i.e 565 kcal for breakfast) set by the nutritional
biologist through the diet configurator (Figure 5);
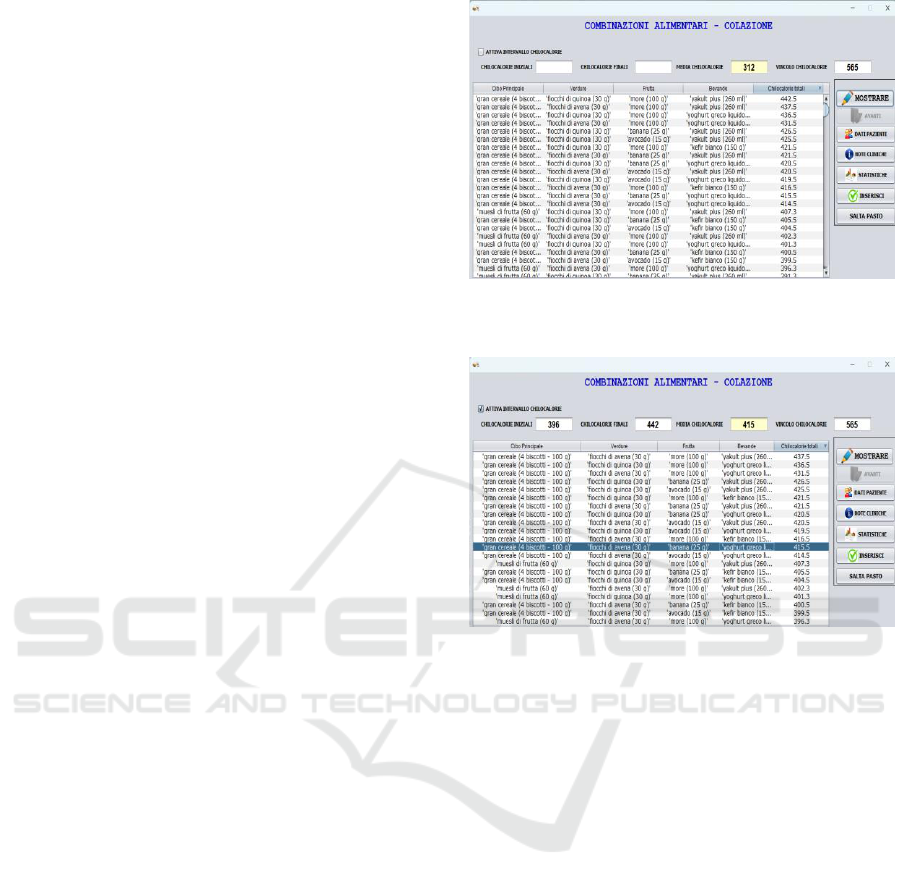
2. First summary evaluation by the nutritional
biologist of the n admissible solutions (n child nodes
of the n-ary tree) based on the objective function (565
kcal for breakfast) and average value (of all food
combination) 312 kcal like heuristic, of all food
combinations (Figure 6);
3. The nutritional biologist sets lower and upper
bounds (operation on the objective function) to avoid
the evaluation of all food combinations of the four
food portions (method not feasible from a
computational point of view) (Figure 7);
4. Evaluation of the optimal feasible solution, f(x*),
in the range of lower (i.e. 396 kcal) and upper (i.e.
442 kcal) bounds of the objective functions and
completed by an integrated step based on a local
search approach that explores a neighborhood N: S
→ N(S) subset of the feasible set S, and determined
by the bounds and the heuristic, the average of food
combinations included in the bounds (i.e. 415 kcal).
In choosing the most suitable food combination for
the specific meal of the day, the nutritional biologist
will be able to take advantage of the clinical
information (histogram of nutrients and glycemic
curve of the combinations) present in the sections
“NOTE CLINICHE” and “STATISTICHE” (to be
viewed in the software demo session – section 2.1) to
evaluate the constraints (cholesterol, fibers,
potassium, sodium, etc.) of each combination of four
portion of food (Figure 7).
5. The food combination chosen for breakfast by the
nutritional biologist is the following: gran cereale (4
biscotti – 100 g) , fiocchi di avena (30 g), banana (25
g) and yoghurt greco liquido (150 g);
6. Iteration of the previous steps for all remaining
meals of the day determined through the diet
configurator (lunch, afternoon snack, and dinner –
Figure 5);
7. Stop criterion (the nutritional biologist chose the
daily food combination).
Note 1 - For the first computational approach, the
"SALTA PASTO" option was programmed which
allows not to consider a combination of food portions
for each of the six programmed meals (breakfast,
morning snack, lunch, afternoon snack, dinner,
evening snack).
Figure 6: Running demo session of the steps 1 and 2 of the
enumerative - heuristic algorithm with constraints.
Figure 7: Running demo session of the steps 3 and 4 of the
enumerative - heuristic algorithm with constraints.
The first heuristic algorithm has been
implemented through a two-dimensional array of real
numbers, double[][] foodmatrix = new double [n][m];
having as rows, n, the portions of the food for the
specific meal to which the relevant kilocalories are
associated, while as the m columns (m=5) the specific
food category (main, food, vegetables, fruit and
drinks) and like last columns the sum of the
kilocalories of the selected food combination. The
second solution approach, based on a combinatorial -
heuristic algorithm with constraints, has been
designed according to three levels of abstraction:
• specific meal planning - corresponds to the
choice of n portions of foods, belonging to the
categories (main food, vegetables, fruit and
drinks), to be taken within a specific meal
(breakfast, morning snack, lunch, afternoon
snack, dinner, and third snack), calibrated for a
single meal;
• planning of the day - corresponds to the choice
of n portions of foods, belonging to the
categories (main food, vegetables, fruit and
drinks), to be taken within the six specific meals
BIOINFORMATICS 2025 - 16th International Conference on Bioinformatics Models, Methods and Algorithms
524
(breakfast, morning snack, lunch, afternoon
snack, dinner and third snack), calibrated for a
day;
• planning of the week - corresponds to the choice
of n portions of foods, belonging to the
categories (main food, vegetables, fruit and
drinks), to be taken within the six specific meals
(breakfast, morning snack, lunch, afternoon
snack, dinner and third snack), calibrated for a
week.
The idea behind the second algorithmic approach
is to adopt an expansion criterion based on the most
"promising" decision in a given step of the problem
to reach an optimal solution for the given meal of the
day, f(x*), compatibly with the constraints imposed
on the nutrients to be respected for the specific diet.
The expansion criterion is updated iteratively to take
into account previously evaluated decisions. The
combinatorial algorithm with constraints created
allows the nutritional biologist to iteratively add, or
not, the portions of food with relative kilocalories
until arriving at a complete solution (expansion
criterion for the specific meal of the day). At each
iteration, the portions of food, with relative
kilocalories, that produces the greatest improvement
in the objective function for the specific meal of the
day is added (automatically determined by the food
regime configurator under the supervision of the
nutritional biologist). This algorithmic approach is
applicable if the solution (a combination of n food
portions for all meals of the day) can be obtained as a
subset of input data (all the possible combination of
m food portions for all meals of the day) – (Figure 8)
Below is the formalization of the data of the second
algorithmic approach:
S.P. = Specific problem (maximization of the
objective function based on kilocalories of food
portions for all meals of the day), established by the
nutritional biologist and evaluated by the diet
configurator with the relative constraints imposed on
nutrients;
S = Set of eligible solutions (food portions for the
specific daily meal: breakfast, morning snack, lunch,
afternoon snack , dinner and evening snack);
S
optimal
= Subset of S, consisting of optimal portions
of food chosen by the nutritional biologist for the
particular diet;
S
partial
= Partial solution for the specific meal of the
day (breakfast, morning snack, lunch, afternoon
snack, dinner, evening snack) chosen by the
nutritional biologist for the particular diet;
Beyond the conceptual scheme of the second
algorithmic approach is the following:
1. Initialize the problem instance S.P.;
2. Evaluate the set of admissible solutions S;
3. For each choice to be made, the nutritional biologist
makes the optimal decisions respecting the nutritional
constraints of the specific problem (S.P.);
4. The criterion for inserting the n portions is
dynamically updated in order to take into account the
choices made previously to determine the partial
solution S
partial
There are two stopping criteria:
1. predetermined number of choices, made by the
biologist nutritionist, for the specific daily meal;
2. obtaining final optimal solution consisting of most
suitable portions of food chosen by the nutritional
biologist for all daily meals.
Beyond the conceptual scheme, it is possible to
formalize the combinatorial- algorithm with
constraints in pseudocode:
INPUT S.P. (Instance of the specific problem)
S ← S
partial
(Initializing partial solution for S.P.)
WHILE S can be extended DO
Find the S
optimal
extension of S: S ← S
optimal
END WHILE
OUTPUT S
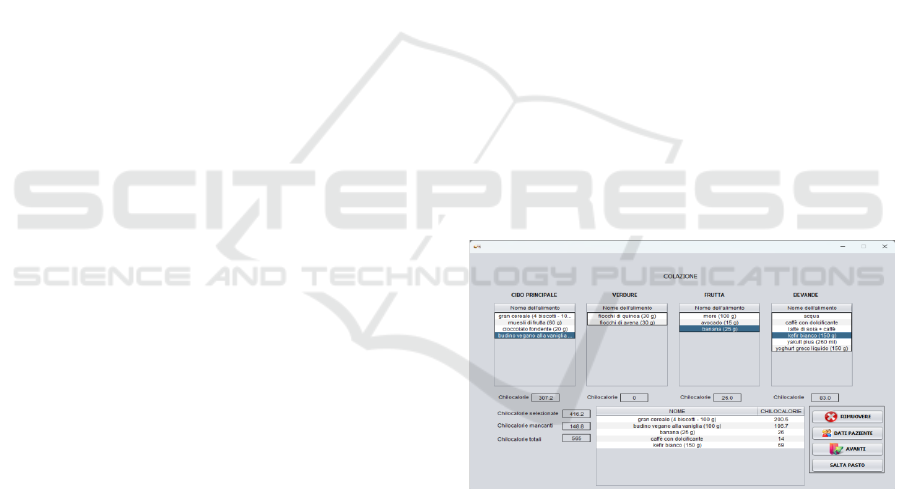
Figure 8: Running demo session of the combinatorial –
heuristic algorithm with constraints.
In the specific case:
S.P. = maximization of the kilocalorie value
established by the diet configurator for the specific
meal (565 kcal for breakfast)
S = totality of the specific clinical choices of the
nutritional biologist based on the food portions
foreseen for the specific meal (breakfast);
S
optimal
= choice by the nutritional biologist of all the
food portions, among the various available , most
suitable for the specific daily meal and for the
particular diet;
System DietadHoc: A Fusion of Human-Centered Design and Agile Development for the Explainability of AI Techniques Based on Clinical
and Nutritional Data
525
S
partial
= gran cereale (4 biscotti – 100 g), budino
vegano alla vaniglia (100 g), banana (25 g) and caffè
con dolcificante e kefir bianco (150 g).
The algorithm was implemented through a
circular queue. In this way the nutritional biologist
can eventually delete [dequeue operation –
Dequeue()] the choice of food portions belonging to
four categories (main food, vegetables, fruit and
drinks). Seeing the demonstration session present in
paragraph 2.1, the nutritional biologist has a real time
evaluation of the update, or modification of the
objective function (kilocalories associated with food
portions for the specific meal) – (Figure 8).
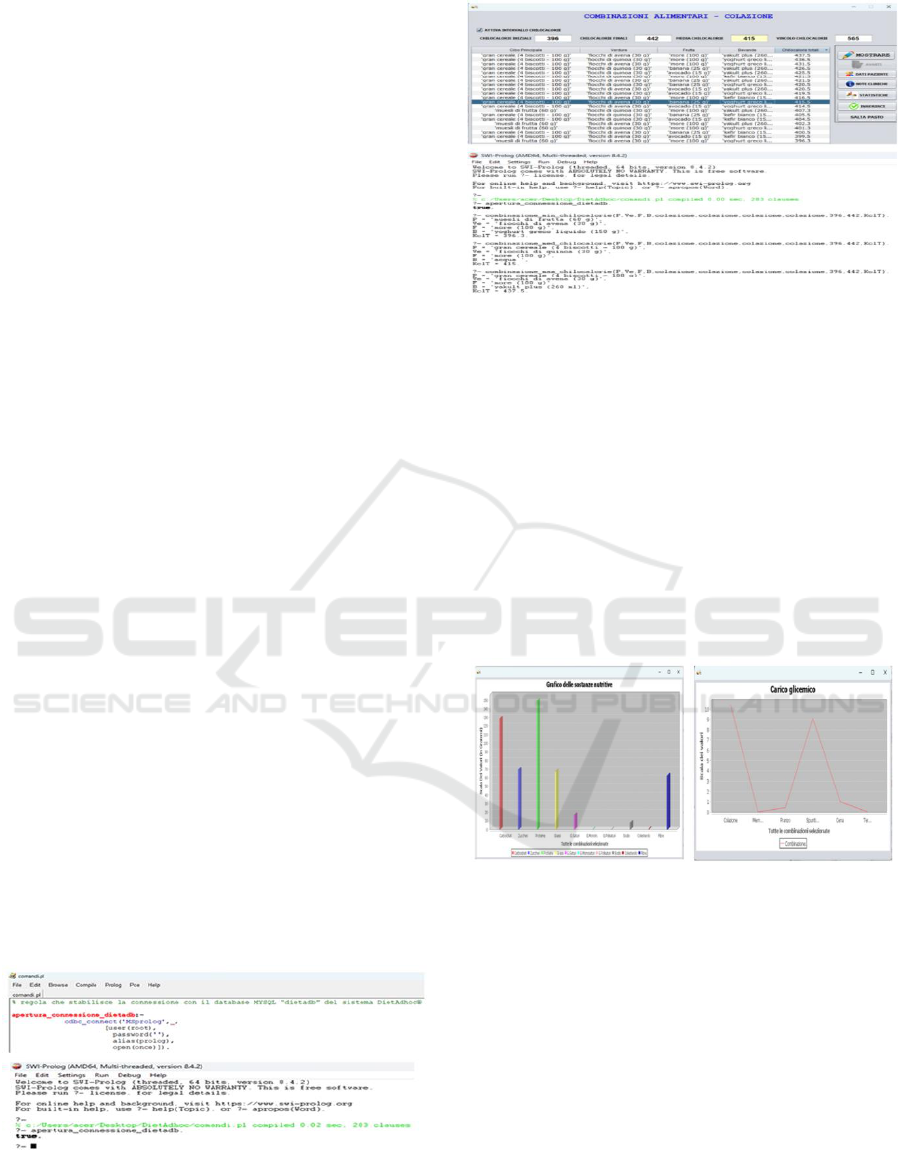
5 DEDUCTIVE DATABASE
In the previous chapters, two heuristic algorithms
were shown that allow the nutritional biologist to
examine various food combinations and determine
the most suitable ones for the specific patient. At the
same time, the DietAdhoc system can have a
symbolic approach. If Prolog programs are
constrained to use only atoms, integers, and reals, and
do not allow recursive rules, you get a powerful
subset of SQL. Under these assumptions, Prolog and
SQL share a core: every query expressible in a subset
of Prolog can in turn be expressed in a subset of SQL,
that means these subsets are logically equivalent
(Warren D.S., 1999).
For this research work, it has been studied the
possibility of interfacing SWI - Prolog with the
DBMS at the basis of the DietAdhoc system through
the ODBC driver (Figure 9), transforming the
relational database underlying the system into a
deductive database. Prolog rules has been created
which allow the connection with the relational
database of the DietAdhoc system, access its tables,
carry out queries (even nested), generate all the
anthropometric parameters of the patient and evaluate
the enumerative - heuristic algorithm (Figure 10).
Figure 9: Connection with the deductive database.
Figure 10: Enumerative - heuristic algorithm in the form of
Prolog rules of a deductive database (corresponding to the
specific Java interface).
6 EXPERIMENTAL RESULTS
For the first and the second algorithmic approaches,
once the nutritional biologist chooses the food
combinations for the particular diet, the system
generates a final daily report in which it is possible to
view all the data obtained with flexible and
customizable user interfaces for the purposes of the
various clinical assessments (Figure 11).
Figure 11: Decision support through various graphical
components.
The nutritional biologist will be able to view the
composition of the macronutrients and micronutrients
of the chosen food combinations via a special
histogram (Figure 11). In the case of the glycemic
curve (Carico glicemico) for the diagnosis of diabetes,
through a time series the Y phenomenon was modeled
through five observations at time t, corresponding to
the six daily meals, with integer t varying from 1 to t.
(Figure 11).
The vector bioelectrical impedance analysis
(BIVA) is a methodology developed in the second half
of the 1990s, which uses vector models and is based
on the electrical properties of tissues without the use
BIOINFORMATICS 2025 - 16th International Conference on Bioinformatics Models, Methods and Algorithms
526

of constants, equations and body weight. These
characteristics, together with the low cost and speed
of execution, make BIVA the type of bioimpedance
analysis most used for all those patients who present
alterations in renal and/or cardiac function, or who
find themselves in conditions of extreme
malnutrition, as well as for cancer and neurodeprived
patients, who may have difficulty interacting
correctly or enduring exams that take too long
(Campa F. et al., 2023). The report includes a
graphical representation (vectors) of the body
resistance and reactance values (Figure 12). This
therefore allows an evaluation of the subject's
hydration and nutrition status independently and
without a mathematical calculation of the data based
on the resistance/reactance detected.
Figure 12: BIVA data.
7 COPYRIGHT
The algorithms implemented and the source code of
the DietAdhoc system are protected by copyright law
(Legislative Decree 518/1192, E.C. Directive 250/91,
Law 747/1994, L.633/1941 Articles 20 and 24).
Anyone who violates the aforementioned regulations
faces civil and criminal sanctions relating to the legal
protection of the DietAdhoc software (Law
248/2000).
8 CONCLUSIONS
Basing on the initial clinical objectives agreed with
the domain expert, it has been demonstrated that two
computational approaches, enhanced by the complete
explanation of the decisions generated, can configure
diets supported by the scientific community
providing an aid to the diagnosis of various eating
disorder with the generation of a complete prediction
model.
Some system upgrades are currently in development:
• Import and integration of biomedical data of a
semi-structured nature (json and xml), and in csv
format into the system DietAdhoc;
• Distributed evolution of software for the creation
of a collaboration network between experts in the
nutrition sector and other specialists;
• Human – Centred AI (HCAI) techniques which
allow to have a complete vision of all the data
generated by the system for the purpose of
clinical choices;
• Insertion of predictive machine learning
algorithms for the exploratory analysis of clinical
and nutritional data;
• Symbiotic Artificial Intelligence (SAI)
techniques for support, without replacing them,
other specialists in human nutrition, and
professionals in the medical field interested in a
scientific collaboration;
• Visual Data Mining techniques to discover
regularities and patterns in patients with similar
ongoing therapies;
In subsequent papers, a framework will be
proposed to accelerate the transfer of artificial
intelligence to clinical contexts and to personalize the
treatment of all nutritional pathologies
REFERENCES
Mastrangelo S., and Boscarol M. (2015) – Linee guida per
la progettazione centrata sull’utente (Versione beta 0.1)
– Gruppo di lavoro per l’usabilità - https://
www.funzionepubblica.gov.it/sites/funzionepubblica.g
ov.it/files/linee_guida_appalti_hcd_beta01_0.pdf
Bhagwat S., Haytowitz D.B and (2010) – USDA Database
for the Oxygen Radical Absorbance Capacity (ORAC)
of selected food – Nutrient Data Laboratory, Beltsville
Human Nutrition Research Center (BHNRC) –
Agricultural Research Service (ARS) - U.S. Department
of Agriculture (USDA) MD May 2010 -
https://www.ars.usda.gov/
ARSUserFiles/80400525/articles/airc07_orac.pdf
Remer and Manz F. – (1995) - Potential renal acid load of
foods and its influence on urine pH - Journal of the
American Dietetic Association Volume 95, Issue 7, July
1995, Pages 791-797 - https://doi.org/10.1016/S0002-
8223(95)00219-7
Mehra A, Starkoff B.E. and Nickerson B. S. (2025) – The
evolution of bioimpedance analysis – Nutrition Volume
129, January 2025, 112601 -
https://doi.org/10.1016/j.nut.2024.112601
Scazzina F., Dall’Asta M. and Casiraghi M.C. (2016) -
Glycemic index and glycemic load of commercial Italian
System DietadHoc: A Fusion of Human-Centered Design and Agile Development for the Explainability of AI Techniques Based on Clinical
and Nutritional Data
527

foods - Nutrition, Metabolism and Cardiovascular
Diseases Volume 26, Issue 5, May 2016, Pages 419-429
– https://doi.org/10.1016/j.numecd.2016.02.013
Warren D.S. (1999) - Prolog as database query language –
Introduction to Prolog (section: deductive database)
https://www3.cs.stonybrook.edu/~warren/xsbbook/nod
e11.html#:~:text=Prolog%20is%20an%20elegant%20l
anguage,a%20powerful%20subset%20of%20SQL.
Campa F., Coratella G., Cerullo G., Stagi S., Paoli S. Marini
S., and Grigoletto A. (2023) - New bioelectrical
impedance vector references and phase angle centile
curves in 4,367 adults: The need for an urgent update
after 30 years https://doi.org/10.1016/j.clnu.2023.
07.025 - Clinical nutrition Volume 42, Issue 9,
September 2023, pages 1749-1758
BIOINFORMATICS 2025 - 16th International Conference on Bioinformatics Models, Methods and Algorithms
528
