Quantifying the Role of Active Listening and Reassurance in Virtual
Health Coach Interactions
Hussain Ghulam
a
, Brian Keegan
b
and Robert Ross
c
ADAPT Centre / School of Computer Science, TU Dublin, Ireland
Keywords:
Conversational Agents, LLM, Health Care, Active Listening, Reassurance.
Abstract:
Conversational Agents have the potential to support healthcare through coaching exercise routines, but are
still lacking in demonstrating authentic social behaviours to support engagement. To this end, we present a
series of experiments that we conducted in order to investigate how automated health care coaches can be
more effective when their interaction style is tailored to demonstrate qualities associated with a good bedside
manner, namely active listening and reassurance. To test this, we first developed a dataset of 135 dialogue
excerpts from three distinct sources, i.e., original, handcrafted and LLMs, the latter two of which were tuned
to demonstrate specific types of comforting or reassuring language. Using this dataset, we conducted a study to
validate whether users perceive different levels of active listening and reassurance across sources. The results
of the study indicate that users can distinctly perceive the varying levels of stimuli across the three different
data sources and that LLMs in particular clearly demonstrate these properties. In an accompanying analysis,
the results showed that there is no notable influence of participant personality on perception, which we argue
reduces the barrier to successful system deployment.
1 INTRODUCTION
Setting exercise goals can positively affect both phys-
ical and mental health, as well as aid recovery and
postoperative care for various medical conditions
(Hallal et al., 2016). The use of conversational agents
(CAs) as intelligent tools to deliver interventions to
achieve exercise goals represents a novel and poten-
tially inclusive approach to broadening physical ac-
tivity. These CAs can, in principle, exhibit greater
adaptability and personalization to user needs and of-
fer personalized recommendations based on prefer-
ences, goals, and fitness levels to improve physical ac-
tivity (Beinema et al., 2021). Despite recent progress
in context-oriented conversation models, integrating
certain language types that are adaptive and engag-
ing remains a challenge, hindering their ability to pro-
vide responses that feel more human-like and exhibit
human level emotional intelligence (Ahmad et al.,
2022).
As a manifestation of demonstrated emotional in-
telligence, good bedside manner in healthcare settings
refers to how healthcare professionals interact with
their clients. Possessing a good bedside manner is
a
https://orcid.org/0009-0000-6256-5523
b
https://orcid.org/0000-0002-7793-398X
c
https://orcid.org/0000-0003-1449-1827
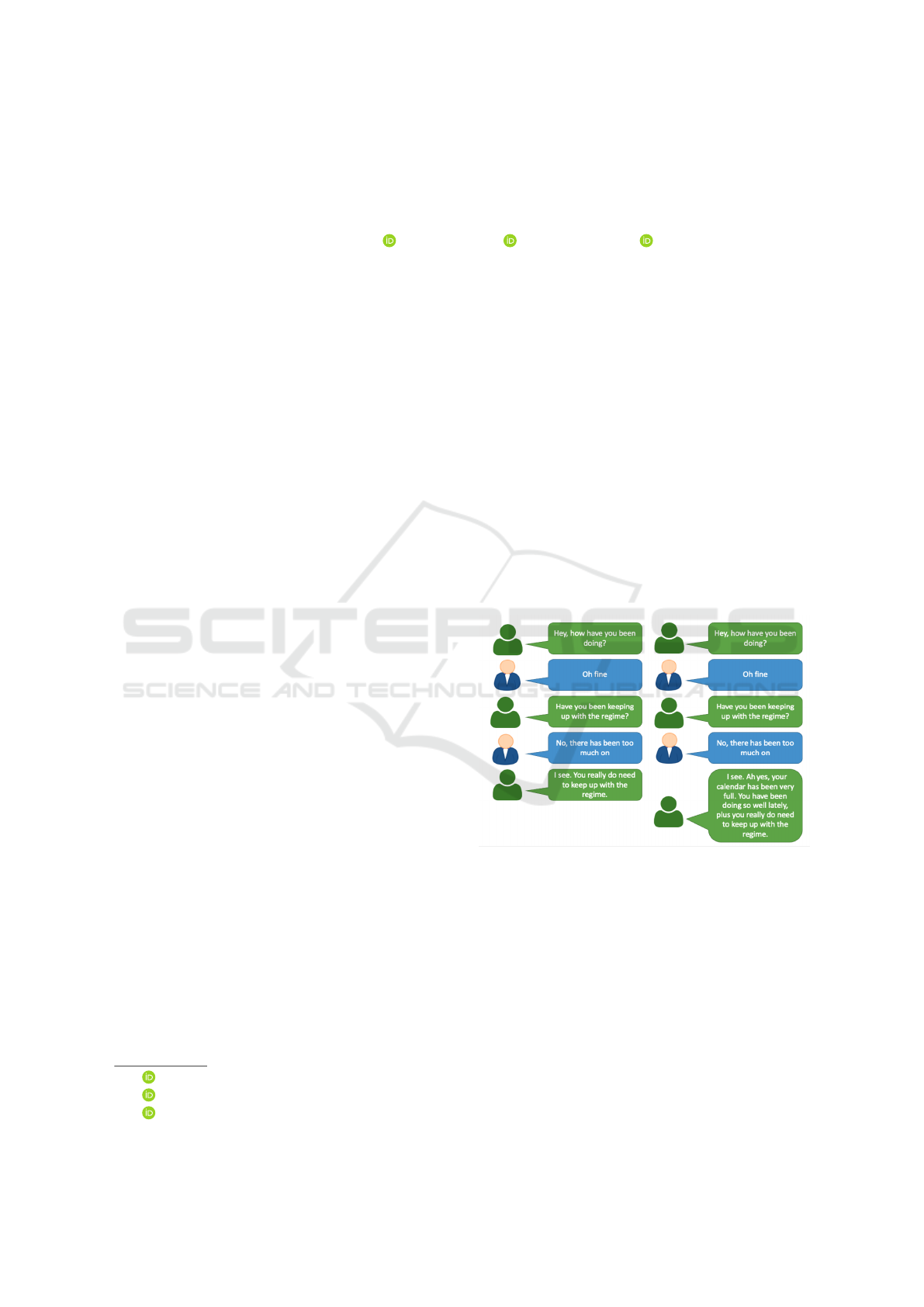
Figure 1: Contrasting Conversational Excerpts: Demon-
strating Presence and Absence of Active Listening and Re-
assurance Behaviors (Right) vs basic form (Left).
assumed to imply that clinicians and related health
professionals are kind, friendly, and understanding of
those in their care (Elliott, 2018). Good bedside man-
ner has been described as characterized by qualities
such as Active Listening and Reassurance (Berman
and Chutka, 2016). To illustrate, an example of two
contrasting interactions is shown in Figure 1. where
the interaction on the right-hand side demonstrates a
higher degree of encouragement, active listening, and
reassurance relative to the more basic form on the left.
Hussain, G., Keegan, B. and Ross, R.
Quantifying the Role of Active Listening and Reassurance in Virtual Health Coach Interactions.
DOI: 10.5220/0013124900003911
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 18th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2025) - Volume 2: HEALTHINF, pages 449-457
ISBN: 978-989-758-731-3; ISSN: 2184-4305
Proceedings Copyright © 2025 by SCITEPRESS – Science and Technology Publications, Lda.
449

Active Listening has been shown to make pa-
tients comfortable and alleviate their fears and anx-
ieties (Fassaert et al., 2007) while reassurance has
been shown to restore confidence, hope, and encour-
ages patients to pursue their goals (Rolfe and Burton,
2013). Despite significant studies that discuss and
emphasize the importance of active listening skills
and reassurance in healthcare education, there re-
mains a notable scarcity of studies that address active
listening and reassuring behaviour from the patient’s
perspective (Snyder, 2008).
In the context of conversational healthcare assis-
tants, the assumption prevails that CAs should display
many of the same qualities associated with a good
bedside manner, such as the ability to listen and com-
fort. However, it is far from clear whether CAs should
exhibit these qualities for all users during healthcare
communication, and indeed, it is much less clear how
these behaviors can and should be fine-tuned to the
user and conversational context.
Considering this, our research focuses on the de-
sign of adaptive-policy strategies (Sahijwani, 2022)
for a CA assisted health coaching system (Beinema
et al., 2023), which supports users in their health-
care goals by demonstrating suitable levels of active
listening and reassurance to the user. We are work-
ing specifically in the domain of exercise regime sup-
port, as this is applicable to a wide range of the pop-
ulation but has particular long-term benefits for the
medical community (Liang et al., 2021a). This pa-
per presents our work on an initial set of experiments
to validate the realization and user perception of be-
havioural variants in interaction to demonstrate the
ability to listen and reassure in typical coaching sce-
narios. The contribution of this work are as follows:
• The construction of a corpus of dialogue ex-
cerpts that demonstrate language types indicative
of active listening and reassuring language in the
health coaching domain.
• An evaluation of whether participants can identify
differences in language types controlled against
the source of that language and participant per-
sonality type.
2 BACKGROUND AND RELATED
WORK
Recently, CAs have been widely used in promoting
physical activity and improving health outcomes in
healthcare (Cohen Rodrigues et al., 2024). In such
cases, CAs provide patients with personalized guid-
ance and motivation to engage in physical activity,
track their progress, and provide feedback on their
performance. Additionally, CAs can be employed to
deliver educational resources to patients on the bene-
fits of physical activity and how to engage in it safely
and effectively (Cohen Rodrigues et al., 2024). It has
also been claimed that the use of CAs to promote
physical activity has the potential to improve overall
health outcomes, prevent chronic diseases, and reduce
healthcare costs (Moore et al., 2023). The existing
studies on the use of CAs in health and well-being
show that the field seems to be in its early stages of
development with some evidence of user acceptance
of CAs in the physical health domain (Wutz et al.,
2023). Despite the promising adoption of CAs in
healthcare, the research indicates a lack of human-like
effective communication and language types (Shan
et al., 2022).
Current health-centric CAs primarily focus on
users’ activity goals—meaning they concentrate on
coaching actions, mainly providing information re-
lated to regime prescription and physical assessment
with little work to date focusing on the social as-
pects of interaction management. However, the use of
social behaviours can help build strong relationships
and user engagement by incorporating different levels
of user personality aspects such as traits, persona and
language styles during communication (Fernau et al.,
2022). Indeed, CAs equipped with certain types of
language as indicators of empathetic language have
been found to play a central role in improving phys-
ical activity by helping people overcome anxiety or
concerns about physical activity (Lynch et al., 2022).
Additionally, such systems have been found to con-
tribute towards building and restoring confidence, fos-
tering a sense of care, and ensuring a feeling of calm.
This, in turn, alleviates doubts and enables people to
feel safe and valued in both clinical and non-clinical
settings (Hicks et al., 2014; Karlsson et al., 2012;
O’Keeffe et al., 2016).
Tuning to the specifics of Active Listening and
Reassurance: in early work Traeger et al. (2017), in-
dicated that reassurance is a notable psychological as-
pect related to good bedside manner which is very
important for various patient groups, including those
with long-term medical conditions and those under-
going pre- and post-treatment, as well as physical
therapy and counseling. Meanwhile, active listening
has been studied by Jagosh et al. (2011) as another
very crucial communicative behavior. This behavior
is valued not only in general communication, but also
in specialized health fields such as nursing, medicine,
health coaching, counseling, and rehabilitation (King,
2021). In the context of physical health, active listen-
ing enables the trainer to transition from being an ‘ex-
HEALTHINF 2025 - 18th International Conference on Health Informatics
450

pert’ to a helpful guide. Instead of exerting pressure,
the trainer assumes the role of a supportive partner,
offering encouraging and reassuring communication
(
´
Olafsson et al., 2019). In active listening-focused
activities, such as counseling, occasional feedback
is essential to maintain a smooth flow of conversa-
tion. Feedback can be achieved by using supporting
backchannel (BC) cues, such as ‘Uh-huh’, ‘mm-hm’,
‘yeah’, ‘okay’ and ‘right’ (Ruede et al., 2017). BCs
serve as verbal and nonverbal indications of attention,
helping the listener to determine when it is their turn
to speak. The listener can incorporate BCs to express
their thoughts without interrupting the speaker (Lala
et al., 2017). There are two types of backchannels:
verbal backchannel, including responses like ‘mm-
hm’, ‘uhh-huh’ and ‘okay’, and nonverbal backchan-
nel, consisting of cues like nodding the head, mak-
ing eye contact, or laughing (Heinz, 1998). Research
indicates that the inclusion of backchannels can en-
hance user engagement and create a more natural con-
versation flow. Additionally, the backchannels con-
tribute to establishing a more positive relationship be-
tween the user and the conversational agent (Ding
et al., 2022).
3 EXPERIMENTAL GOALS AND
DESIGN
Given the lack of systematic investigation on this
topic to date, the present study seeks to investigate
methods to manipulate levels of reassurance and ac-
tive listening in CA output, and measure whether text
designed to demonstrate active listening and reassur-
ance was perceived as such by analyzing participant’s
perceptions of the provided texts. Our goal therefore
is to provide an approximate calibration of these qual-
ities and measurement of automatically versus manu-
ally collected data.
The experimental design of this study was struc-
tured into three elements:
In the first element, we measured the users’ per-
ception of different levels of active listening and reas-
surance across a corpus of dialogue excerpts sourced
from three distinct pools, i.e., original, handmade, and
LLM-generated content.
The second element of the study aimed to vali-
date whether participants can effectively discern dif-
ferences among language types while controlling for
variations in the source of language. The data sources
were further broken down into Block A (Active Lis-
tening), Block B (Reassurance) and Block C (Neutral)
within each language source.
In the third element of this study, we validated
whether different personality types have any differ-
ences in their perception of active listening and reas-
surance.
3.1 Data Synthesis and Properties
Given a lack of suitable existing data sets, we devel-
oped a dataset of dialogue excerpts clearly stating that
the coach is a conversational agent rather than a hu-
man. Specifically, we built a data set comprising 135
dialogues within the healthcare domain. The data set
has 45 dialogues sourced from original real world in-
teractions, 45 dialogues crafted by human annotators
(handcrafted), and an additional 45 dialogues gener-
ated using an LLM (LLM).
For the original dialogue data, we utilized an ex-
isting open-source dataset comprising human-human
dialogues in the context of physical healthcare coun-
seling to ensure the inclusion of real-world complex-
ities, clients concerns, and diverse language usage.
This data set was collected from a real world physical
activity intervention program for women (Liang et al.,
2021b). This original dialogue dataset was not classi-
fied in any way into active listening and reassurance
as this dataset was aimed to support social support for
physical activity and its barriers.
Building on this real world sourced dataset, hand-
made dialogues were curated with the help of anno-
tators to simulate various physical healthcare scenar-
ios, such as to incorporate a range of medical condi-
tions, and communication styles. For this work we
followed the guidelines and instructions discussed by
Wu et al. (2023). The curated dataset was distributed
proportionally across three blocks: 15 dialogues were
stylised or biased towards active listening, 15 towards
reassurance, and 15 featuring neutral language.
To generate automatic data, we used ChatGPT
3.5 with different prompts to create dialogue excerpts
in specific styles, depicting qualities related to ac-
tive listening and reassurance. The designed prompts
are provided in the appendix for reference. The
LLM-generated excerpts were distributed across three
blocks: 15 styled with active listening, 15 styled to-
wards reassurance, and 15 featuring neutral stimuli.
The data resources from this study are publicly avail-
able to promote further research on GitHub.
1
3.2 Study Design
After collecting the datasets, we conducted three sur-
veys – one for each data source – for dialogue eval-
uation. The surveys included a total of six questions,
1
The data resources are available on Github.
Quantifying the Role of Active Listening and Reassurance in Virtual Health Coach Interactions
451

specifically focused on examining the perception of
active listening and reassurance. The first three ques-
tions assessed active listening, while the remaining
three questions referred to reassurance. A 5-point
Likert scale was used to assess participant responses.
The participant ratings were calculated by averaging
the responses from each segment, reflecting perceived
levels of active listening and reassurance. These ques-
tions are included in the appendix for reference.
Nine dialogues were randomly displayed for each
user interaction. The evaluation system was deployed
on the Prolific crowd-sourcing platform (Eyal et al.,
2021) with informed consent. The time allotted to
each participant was 20 minutes. In total 90 partic-
ipants were recruited; 30 for each of the 3 language
sources, original, handmade, and LLM dialogues.
Following the stimuli rating activity, we asked
participants to rate themselves against the ten item
personality measure (TIPI) personality test (Gosling
et al., 2003) to assess the different personality lev-
els of participants. This supplementary assessment
aimed to validate whether different types of person-
ality have different trends regarding the perception of
active listening and reassurance. This measurement
results in an estimate of the openness, conscientious-
ness, extroversion, agreeableness, and emotional sta-
bility of the Big 5 personality traits demonstrated by
each participant.
3.3 Participant Demographics
In the first survey, which focused on data from origi-
nal dialogues, the cohort of 30 participants included
10 males, 17 females, and 3 participants who pre-
ferred not to disclose their gender. The ages of the
participants ranged from 22 to 67 years (M = 38.4,
SD = 5.63). The second survey, centered on hand-
made dialogues, included 14 men and 16 women in
the 30-participant cohort, with ages ranging from 23
to 73 years (M = 39.11, SD = 6.22). In the third sur-
vey with LLM-generated data, which also featured
30 participants, there were 12 men and 18 women,
and the age range was 27 to 55 years (M = 39.72,
SD = 6.16). Participants from the US, UK, Ireland,
New Zealand, and Australia were sourced across the
three studies. Analyzing the median time participants
spent engaging with the experiments reveals notable
patterns. The median time taken by participants in
survey I was approximately 17.68 minutes. Survey
II reveals that the median time taken by participants
was approximately 16.91 minutes. Survey III how-
ever stands out with a significantly shorter median
time of 9 minutes. The main cause of this shorter me-
dian time may be the ease of linguistic styles mim-
Figure 2: User’s Perception of Active Listening across Lan-
guage Sources (original, handmade, LLM).
Figure 3: User’s Perception of Reassurance across Lan-
guage Sources (original, handmade, LLM).
icked by LLMs, However, it can be in part be at-
tributed to average dialogue length. The mean lengths
of dialogues vary across data sources, with the dataset
of original dialogues having the longest dialogues
(mean length: 270.82 tokens), the handmade dataset
exhibiting moderate lengths (mean length: 215.59 to-
kens), LLM-generated dialogues feature the shortest
dialogues (mean length: 106.18 tokens).
4 EXPERIMENTAL RESULTS
In this section, we present the experimental results for
the three elements of the study.
HEALTHINF 2025 - 18th International Conference on Health Informatics
452
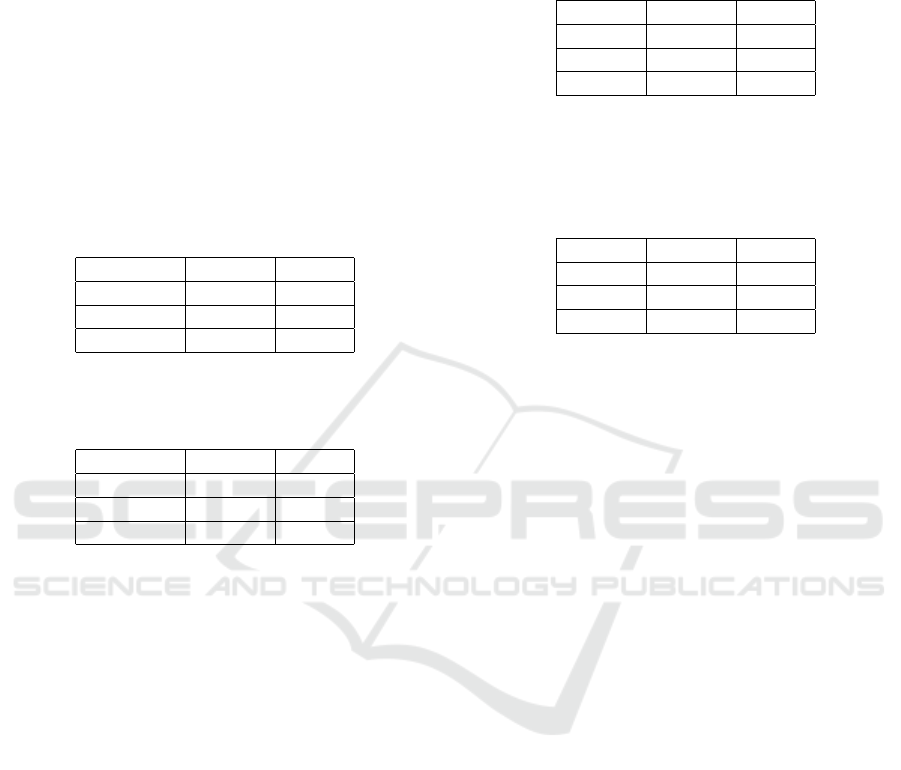
4.1 Source Analysis
The first element investigates the perception of active
listening and reassurance across the three language
sources: original, handcrafted, and LLM-Generated
dialogues. Our goal here is to determine as a baseline
whether participants perceived any variation in over-
all amounts of reassurance and active listening across
the sources without taking into account any styling
blocks within those sources. Figures 2 and 3, illus-
trate the Likert scale ratings of perceived active lis-
tening and reassurance provided by the participants.
Table 1: Anova with post-hoc Tukey’s HSD Results for
Overall User’s Perception of Active Listening across the
data sources (original, handmade, LLM).
Group 1 Group 2 p-adj
Handmade LLM 0.9295
Handmade original 0.5448
LLM original 0.3347
Table 2: Anova with post-hoc Tukey’s HSD Results for
Overall User’s Perception of Reassurance across the data
sources (original, handmade, LLM).
Group 1 Group 2 p-adj
Handmade LLM 0.9437
Handmade original 0.3586
LLM original 0.5485
Overall, the results show that users perceive ac-
tive listening and reassurance slightly higher in both
the LLM and Handcrafted dialogues than in the base-
line original content. The perceived level is strongest
in LLMs. These results can be explained by the fact
that original content was not purposefully designed to
have reassurance and active listening qualities while
the other two text sources were designed (in part) to
display these styles. Statistical analysis by means of
the Anova with post-hoc Tukey’s HSD in Tables 1 and
2 shows that there are no statistically significant dif-
ferences in mean perception scores for ‘Active Lis-
tening’ and ‘Reassurance’ between any of the com-
pared language sources (‘Original’, ‘Handmade’, and
‘LLM-Generated’) and the adjusted p-value is also
recorded greater than the significance level. This in it-
self is also aligned with our experimental design since
not all dialogue examples within the LLM and hand-
crafted sets were stylised, thus resulting in a small and
notable though not strong perception effect.
4.2 Style Analysis
To dig deeper and account for the specific stylistic
biasing of the individual dialogues, the second ele-
Table 3: Anova with post-hoc Tukey’s HSD results for the
Perception of Active Listening Across the different blocks
of Handmade Data. Block A = Active Listening biased data;
Block B = Reassurance biased data, and Block C = Neutral
data.
Group 1 Group 2 p-adj
Block A Block B 0.6812
Block A Block C 0.7777
Block B Block C 0.9858
Table 4: Anova with post-hoc Tukey’s HSD results for the
Perception of Reassurance Across the different blocks of
Handmade Data. Block A = Active Listening biased data;
Block B = Reassurance biased data, and Block C = Neutral
data.
Group 1 Group 2 p-adj
Block A Block B 0.8019
Block A Block C 0.7262
Block B Block C 0.9907
ment of the investigation aimed to validate the partici-
pant ratings of active listening and reassurance against
the breakdown of the 45 dialogues distributed across
three distinctively styled blocks: Block A (Active
Listening biased data), Block B (Reassurance biased
data), and Block C (Neutral). We present results for
handmade dialogues and LLM dialogues but not orig-
inal content since no style biasing was applied for that
content.
Handmade Dialogues: For handmade dialogues, as
depicted in Figure 4, for the perception of Active Lis-
tening (blue) we can see that participants identified
slightly more active listening in the active listening
biased data Block A than was the case for the neutral
data Block C. Similarly for the perception of reassur-
ance (green), participants perceived slightly greater
levels of reassurance on average in reassurance biased
data than was the case for the neutral data Block C. In
both cases however the effect is not strong, and statis-
tical tests shown in Table 3 demonstrate that the effect
was not significant across blocks. It is also notable
that reassurance and active listening perceptions cross
bias blocks are very similar. In other words partici-
pants see reassurance in Active Listening biased data
and see Active Listening in Reassurance biased data.
Though the reported values were lower, it is notable
here that the users perceived active listening and re-
assurance even in the neutral Block C data. This may
be due to various factors such as tone, context, and
non-verbal cues. In fact, language does not necessar-
ily eliminate all the cues that can influence the per-
ception of active listening or assurance, as no effort
was made to actively engineer this out of the baseline
dialogues.
Quantifying the Role of Active Listening and Reassurance in Virtual Health Coach Interactions
453
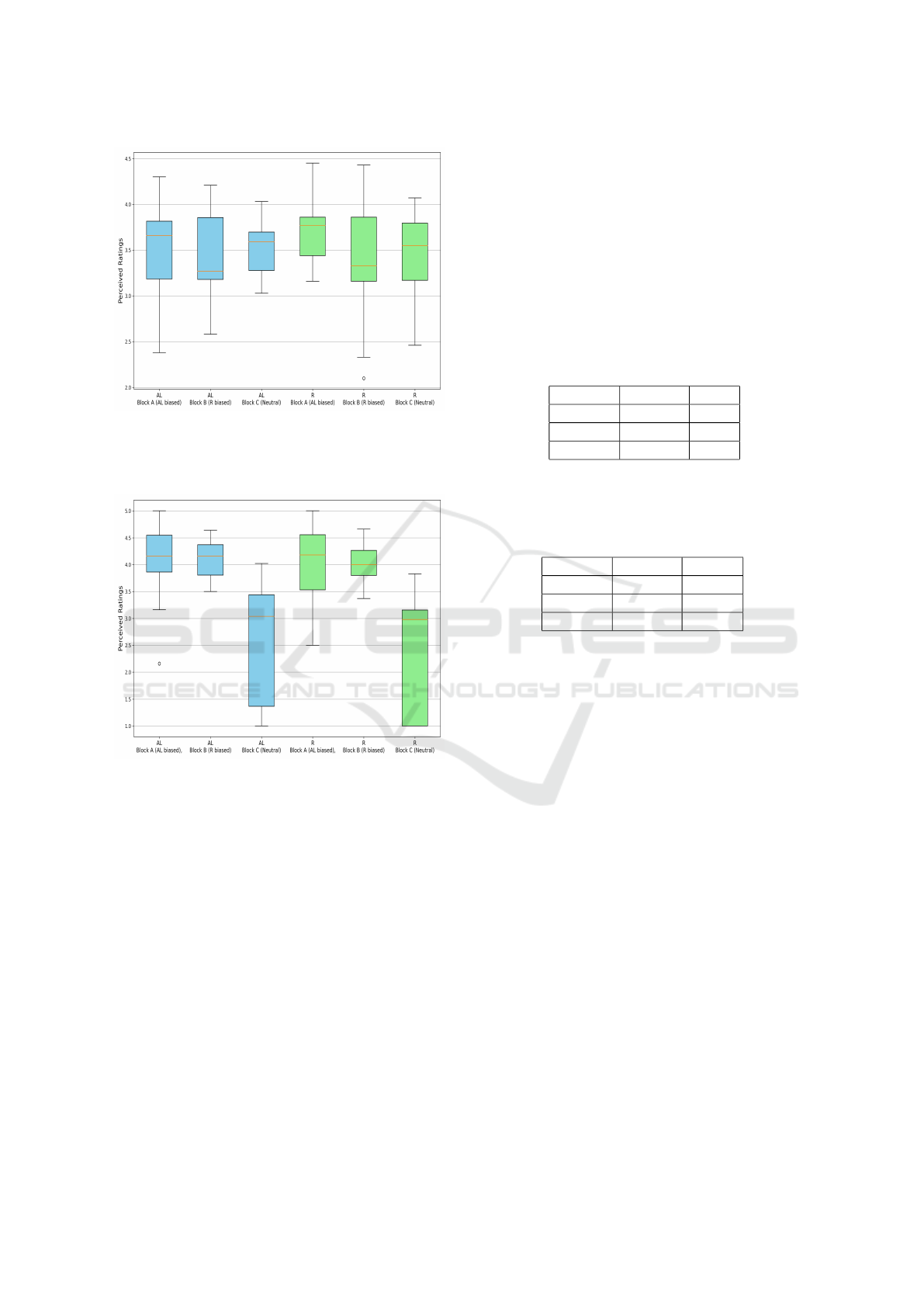
Figure 4: User Perception of Active Listening (Blue) and
Reassurance (Green) across Handmade Content. Block A
(Active Listening), Block B (Reassurance) and Block C
(Neutral).
Figure 5: User’s Perception of Active Listening (Blue)
and Reassurance (Green) across LLM-Generated Content.
Block A (Active Listening), Block B (Reassurance) and
Block C (Neutral).
LLM Generated Data: Turning to the LLM data,
Figure 5 presents a similar analysis for the LLM data.
Generally the results follow the same overall pattern
as those for the handcrafted content, but with a much
clearer distinction between the perception results for
neutral dialogues versus the dialogues that were bi-
ased towards reassurance and active listening. As was
the case for handcrafted dialogues, again we see that
participants do in fact perceive high values of active
listening in dialogues which were biased for reassur-
ance, and vice versa. While comparing to those re-
sults for the handcrafted dialogues, it is clear that the
measures of reassurance and active listening are in-
stinctively clearer for LLM generated data than hand-
crafted dialogue. Statistical analysis by means of
Anova with post-hoc Tukey’s HSD shows significant
differences in both active listening and reassurance
perceptions across the experimental blocks. These
findings underscore the potential of the engineered
stimuli successfully influencing perceptions of active
listening and reassurance. Tables 5 and 6 show the
detailed results of the Anova with post-hoc Tukey’s
HSD Test across the 3 blocks.
Table 5: Anova with post-hoc Tukey’s HSD Test Results
for the perception of Active Listening across the different
blocks of LLM-Generated Data. Block A (Active Listen-
ing), Block B (Reassurance) and Block C (Neutral).
Group 1 Group 2 p-adj
Block A Block B 1.0
Block A Block C 0.0
Block B Block C 0.0
Table 6: Anova with post-hoc Tukey’s HSD Test Results
for the Perception of Reassurance Across the Different
Blocks of LLM-Generated Data. Block A (Active Listen-
ing), Block B (Reassurance) and Block C (Neutral).
Group 1 Group 2 p-adj
Block A Block B 0.9986
Block A Block C 0.0
Block B Block C 0.0
4.3 Personality Variance in Perception
While it is interesting to understand whether the over-
all population can perceive of active listening and re-
assurance in designed content, it is important to rec-
ognize the potential for individual differences. There-
fore, we also collected personality measures to ana-
lyze whether personality traits correlate with the per-
ceptions of active listening and reassurance for each
participant in the LLM-generated content.
We present this analysis for the LLM sourced data.
As shown in the previous section the perceptions of
active listening and reassurance were most strongly
pronounced in this data, which in turn makes the in-
teractions with personality traits most valid for inves-
tigation. Our hypothesis is the existence of a linear
relationship between elements of personality measure
and perception measures of active listening and reas-
surance, To measure the strength and direction of the
this relationship we used Pearson’s correlation coeffi-
cient (r). Since different participants reviewed stimuli
across three stylistic blocks, we present the results for
these stylistic blocks individually. Table 7 summa-
rizes these results.
HEALTHINF 2025 - 18th International Conference on Health Informatics
454

Table 7: Pearson Correlation Coefficient (r) between personality traits and blocks with active listening, reassurance biased
and neutral data. AL= Active Listening, R= Reassurance, *p values < 0.01 and **p < 0.05.
Personality Trait
Active Listening biased data Reassurance biased data Neutral data
AL R AL R AL R
Openness 0.2590 0.2599 0.0128 0.0128 -0.0783 -0.1623
Conscientiousness -0.0023 -0.0069 0.0993 0.0457 0.2610 0.1638
Extroversion 0.3977
**
0.2676 -0.4674
*
-0.5339
*
0.0017 -0.1054
Agreeableness 0.2218 0.2596 0.0923 -0.1859 -0.0622 -0.0432
Emotional Stability 0.3937
**
0.3765
**
-0.0622 -0.0051 0.0138 -0.0437
5 DISCUSSION
Our analysis suggests that when dialogues are con-
sciously crafted with language styles that indicate ac-
tive listening and reassurance, users are more likely
to perceive these dialogues as demonstrating those
traits compared to dialogues lacking such intentional
linguistic and social behavior cues. Our study re-
veals that users consistently perceived higher levels
of Active Listening and Reassurance in content gen-
erated by LLMs compared to hand-crafted data. This
discrepancy can likely be attributed to the advanced
content generation capabilities of LLMs when guided
by specific directives and instructions. Additionally,
it is crucial to acknowledge the possibility that user
comprehension may have been hindered during the
creation of hand-crafted data due to potential limita-
tions or inadequacies in conveying the intended lan-
guage styles. In either case the findings suggest that
we can comfortably use LLM generated content that
is tuned to the factors associated with good bedside
manner, and in fact these systems may be better at
consistently demonstrating these qualities than a hu-
man consciously aiming to replicate these styles.
While our study did not demonstrate any strong rela-
tionship between personality traits and the perception
of properties associated with good bedside manner,
that is a positive thing from the perspective of effec-
tive design of health supporting systems in the long
run. The results suggest that we do not need to over-
think the design of these stylistic factors and that with
respect to these elements of support, a one size fits
all approach to displaying support may be sufficient
rather than a dynamic style which needs to be cus-
tomized to individual personality traits.
6 CONCLUSION AND FUTURE
DIRECTIONS
Whilst past studies on Virtual Health Coaching Assis-
tants have emphasised the positive impact of certain
tasks mainly providing information related to regime
prescription and physical assessment, little has been
known about focusing on the social aspects of inter-
action management, To address this gap, our study
focused on inclusion and measuring of social be-
haviours, namely active listening and reassurance, in
the context of system-initiated virtual health coaching
assistants. By building and analysing a dataset com-
prised of 135 dialogues, including original, handmade
and LLM-generated excerpts curated with language
styles related to these qualities, we observed that users
with diverse personality traits perceived varying lev-
els of active listening and reassurance. Our findings
underscore the importance of integrating these social
behaviors into virtual health coaching assistants. This
study laid the foundation work for filling the gap in
understanding and leveraging such behaviors, paving
the way for the development of virtual health coach-
ing prototypes that prioritize active listening and re-
assurance.
Building upon these findings, our future research en-
deavors focuses on developing a virtual health coach-
ing prototype that incorporates varying degrees of ac-
tive listening and reassurance, and validating that dis-
playing these qualities in a controlled way in fact is
beneficial to the participants. Through rigorous exper-
iments, our aim is to determine whether these qual-
ities indeed enhance engagement and effectiveness
compared to systems lacking these qualities. Ulti-
mately, our work aims to contribute to the advance-
ment of virtual health coaching, offering more per-
sonalized and adaptive interventions.
Quantifying the Role of Active Listening and Reassurance in Virtual Health Coach Interactions
455

ACKNOWLEDGEMENTS
This research was conducted with the financial sup-
port of Science Foundation Ireland / Research Ire-
land under Grant Agreement No. 13/RC/2106 P2 at
ADAPT, the SFI Research Centre for AI-Driven Digi-
tal Content Technology. For the purpose of Open Ac-
cess, the authors have applied a CC BY public copy-
right licence to any Author Accepted Manuscript ver-
sion arising from this submission..
REFERENCES
Ahmad, R., Siemon, D., Gnewuch, U., and Robra-Bissantz,
S. (2022). Designing personality-adaptive conversa-
tional agents for mental health care. Information Sys-
tems Frontiers, 24.
Beinema, T., op den Akker, H., Hermens, H. J., and van
Velsen, L. (2023). What to discuss?—a blueprint
topic model for health coaching dialogues with con-
versational agents. International Journal of Hu-
man–Computer Interaction, 39(1):164–182.
Beinema, T., op den Akker, H., van Velsen, L., and
Hermens, H. (2021). Tailoring coaching strategies
to users’ motivation in a multi-agent health coach-
ing application. Computers in Human Behavior,
121:106787.
Berman, A. and Chutka, D. (2016). Assessing effective
physician-patient communication skills: ”are you lis-
tening to me, doc?”. Korean journal of medical edu-
cation, 28.
Cohen Rodrigues, T. R., de Buisonj
´
e, D. R., Reijnders,
T., Santhanam, P., Kowatsch, T., Breeman, L. D.,
Janssen, V. R., Kraaijenhagen, R. A., Atsma, D. E.,
and Evers, A. W. (2024). Human cues in ehealth to
promote lifestyle change: An experimental field study
to examine adherence to self-help interventions. In-
ternet Interventions, 35:100726.
Ding, Z., Kang, J., HO, T. O. T., Wong, K. H., Fung, H. H.,
Meng, H., and Ma, X. (2022). Talktive: A conversa-
tional agent using backchannels to engage older adults
in neurocognitive disorders screening.
Elliott, M. (2018). Good bedside manner. Online.
Eyal, P., David, R., Andrew, G., Zak, E., and Damer, E.
(2021). Data quality of platforms and panels for online
behavioral research. Behavior Research Methods, 54.
Fassaert, T., Dulmen, A., Schellevis, F., and Bensing,
J. (2007). Active listening in medical consulta-
tions: Development of the active listening observation
scale (alos-global). Patient education and counseling,
68:258–64.
Fernau, D., Hillmann, S., Feldhus, N., Polzehl, T., and
M
¨
oller, S. (2022). Towards personality-aware chat-
bots. In Lemon, O., Hakkani-T
¨
ur, D., Li, J. J.,
Ashrafzadeh, A., Garc
´
ıa, D. H., Alikhani, M.,
Vandyke, D., and Dusek, O., editors, Proceedings of
the 23rd Annual Meeting of the Special Interest Group
on Discourse and Dialogue, SIGDIAL 2022, Edin-
burgh, UK, 07-09 September 2022, pages 135–145.
Association for Computational Linguistics.
Gosling, S. D., Rentfrow, P. J., and Swann Jr, W. B. (2003).
A very brief measure of the big-five personality do-
mains. Journal of Research in personality, 37(6):504–
528.
Hallal, P. C., Andersen, L. B., Gonc¸alves, L. G., Wells, J. C.,
Reichert, F. F., Anjos, L. A. d., Ferreira, R. C., and
Victora, C. G. (2016). Physical activity and inactivity
profiles in brazilian adults: results from the national
health survey (pns 2013). Revista de sa
´
ude p
´
ublica,
50:1S.
Heinz, B. M. (1998). Backchannel responses as conversa-
tional strategies in bilingual speakers’ conversations.
The University of Nebraska-Lincoln.
Hicks, K. M., Cocks, K., Martin, B. C., Elton, P. J., Macnab,
A., Colecliffe, W., and Furze, G. (2014). An interven-
tion to reassure patients about test results in rapid ac-
cess chest pain clinic: a pilot randomised controlled
trial. BMC Cardiovascular Disorders, 14.
Jagosh, J., Donald Boudreau, J., Steinert, Y., MacDon-
ald, M. E., and Ingram, L. (2011). The impor-
tance of physician listening from the patients’ per-
spective: Enhancing diagnosis, healing, and the doc-
tor–patient relationship. Patient Education and Coun-
seling, 85(3):369–374.
Karlsson, V., Forsberg, A., and Bergbom, I. (2012). Com-
munication when patients are conscious during respi-
rator treatment—a hermeneutic observation study. In-
tensive and Critical Care Nursing, 28(4):197–207.
King, G. (2021). Central yet overlooked: engaged and
person-centred listening in rehabilitation and health-
care conversations. Disability and rehabilitation,
44:1–13.
Lala, D., Milhorat, P., Inoue, K., Ishida, M., Takanashi, K.,
and Kawahara, T. (2017). Attentive listening system
with backchanneling, response generation and flexible
turn-taking. In Proceedings of the 18th Annual SIG-
dial Meeting on Discourse and Dialogue, pages 127–
136, Saarbr
¨
ucken, Germany. Association for Compu-
tational Linguistics.
Liang, K.-H., Lange, P., Oh, Y. J., Zhang, J., Fukuoka, Y.,
and Yu, Z. (2021a). Evaluation of in-person counsel-
ing strategies to develop physical activity chatbot for
women. arXiv preprint arXiv:2107.10410.
Liang, K.-H., Lange, P., Oh, Y. J., Zhang, J., Fukuoka, Y.,
and Yu, Z. (2021b). Evaluation of in-person counsel-
ing strategies to develop physical activity chatbot for
women. In Li, H., Levow, G.-A., Yu, Z., Gupta, C.,
Sisman, B., Cai, S., Vandyke, D., Dethlefs, N., Wu, Y.,
and Li, J. J., editors, Proceedings of the 22nd Annual
Meeting of the Special Interest Group on Discourse
and Dialogue, pages 32–44, Singapore and Online.
Association for Computational Linguistics.
Lynch, J., Hughes, G., Papoutsi, C., Wherton, J., and
A’Court, C. (2022). “it’s no good but at least i’ve
always got it round my neck”: A postphenomeno-
logical analysis of reassurance in assistive technology
use by older people. Social Science and Medicine,
292:114553.
HEALTHINF 2025 - 18th International Conference on Health Informatics
456

Moore, R., Al-Tamimi, A.-K., and Freeman, E. (2023). A
conversational agent (phyllis) to support adolescent
health and overcome barriers to physical activity: a
co-design and evaluation study (preprint). JMIR For-
mative Research, 8.
O’Keeffe, M., Cullinane, P., Hurley, J., Leahy, I., Bunzli,
S., O’Sullivan, P. B., and O’Sullivan, K. (2016). What
Influences Patient-Therapist Interactions in Muscu-
loskeletal Physical Therapy? Qualitative Systematic
Review and Meta-Synthesis. Physical Therapy, 96(5).
´
Olafsson, S., O’Leary, T. K., and Bickmore, T. W. (2019).
Coerced change-talk with conversational agents pro-
motes confidence in behavior change. Proceedings of
the 13th EAI International Conference on Pervasive
Computing Technologies for Healthcare.
Rolfe, A. and Burton, C. (2013). Reassurance after diag-
nostic testing with a low pretest probability of serious
disease. JAMA internal medicine, 173:1–9.
Ruede, R., M
¨
uller, M., St
¨
uker, S., and Waibel, A. (2017).
Yeah, right, uh-huh: A deep learning backchannel pre-
dictor.
Sahijwani, H. (2022). Adaptive dialogue management for
conversational information elicitation. In Proceedings
of the 45th International ACM SIGIR Conference on
Research and Development in Information Retrieval,
pages 3495–3495.
Shan, Y., Ji, M., Xie, W., Qian, X., Li, R., Zhang, X.,
and Hao, T. (2022). Language use in conversa-
tional agent–based health communication: System-
atic review. Journal of Medical Internet Research,
24:e37403.
Snyder, U. (2008). The doctor-patient relationship ii: Not
listening. Medscape journal of medicine, 10:294.
Traeger, A., O’Hagan, E., Cashin, A., and Mcauley, J.
(2017). Reassurance for patients with non-specific
conditions – a user’s guide. Brazilian Journal of Phys-
ical Therapy, 21.
Wu, Z., Balloccu, S., Kumar, V., Helaoui, R., Refor-
giato Recupero, D., and Riboni, D. (2023). Cre-
ation, analysis and evaluation of annomi, a dataset of
expert-annotated counselling dialogues. Future Inter-
net, 15(3).
Wutz, M., Hermes, M., Winter (n
´
ee Hinz), V., and
Koeberlein-Neu, J. (2023). Factors influencing the ac-
ceptability, acceptance and adoption of conversational
agents in healthcare: An integrative review (preprint).
Journal of Medical Internet Research, 25.
APPENDIX
A: Survey Questions
Research survey included a total of six questions,
specifically focused on examining the perception of
active listening and reassurance. The first three ques-
tions assessed active listening, while the remaining
three questions referred to reassurance.
1. How well did therapist demonstrate active listen-
ing by paying attention and showing interest in
clients concerns?
2. Did the therapist ask questions or provide feed-
back that demonstrated understanding and active
listening?
3. Did the therapist give cues or responses that
showed they were actively listen and paying at-
tention?
4. Did the therapist acknowledge and validate the
client’s concerns or emotions that demonstrated
reassurance?
5. How well did the therapist provide reassurance,
comfort, support, or encouragement to the client?
6. How effective was the therapist in fostering a
sense of reassurance and encouragement for the
client’s overall progress?
B: Designed Prompts
To generate synthetic data, we used ChatGPT 3.5
with different prompts to generate dialogue excerpts
in specific styles, which depicts qualities related to
active listening and reassure.
• Write a dialogue where the therapist actively lis-
tens to the client’s concerns about their progress
in therapy and reassures them with empathy and
understanding
• Craft a scenario where the client expresses anx-
iety about their ability to recover fully, and the
therapist listens attentively while providing reas-
surance and support
• Imagine a dialogue between a therapist and a
client where the client expresses frustration with
their current treatment plan. How does the ther-
apist respond with active listening and reassur-
ance?
• Create a conversation where the client shares their
fears about returning to activities that caused their
injury, and the therapist responds by actively lis-
tening and offering reassurance and guidance
• Write a dialogue where the client discusses feel-
ings of self-doubt and uncertainty about their
progress, and the therapist responds by validating
their concerns and providing reassurance.
Quantifying the Role of Active Listening and Reassurance in Virtual Health Coach Interactions
457
