
Adjusting Doctor’s Reliance on AI Through Labeling for Training Data
and Modification of AI Output in a Muscle Tissue Detection Task
Keito Miyake
1,2 a
, Kumi Ozaki
3 b
, Akihiro Maehigashi
4 c
and Seiji Yamada
2,1 d
1
Informatics Course, The Graduate University for Advanced Studies (SOKENDAI), Kanagawa, Japan
2
National Institute of Informatics, Tokyo, Japan
3
Hamamatsu University School of Medicine, Shizuoka, Japan
4
Shizuoka University, Shizuoka, Japan
Keywords:
Reliance Rate, Artificial Intelligence, Radiology, Human-AI Interaction.
Abstract:
Due to the significant advancements in artificial intelligence(AI), AI technologies are increasingly providing
support in various fields. However, even if AI performs at a high level, humans refuse AI for no obvious
reason and prefer to solve problems on their own. For instance, experts such as medical professionals tend to
be more reluctant to rely on a medical AI’s diagnosis than on a human medical professional. This tendency
leads to undertrust in AI and could affect its implementation in society. Thus, this study aims to mitigate the
undertrust in AI by providing two functions from the perspective of interaction design: (a) labeling AI outputs
as correct or incorrect for training data and (b) modifying AI outputs. To evaluate the effectiveness of these
two functions in increasing medical professionals’ reliance on AI, we conducted an experiment involving 25
radiologists and radiographers participating in a muscle-tissue-detection task. A two-way analysis of variance
was conducted to analyze their AI-usage rate. The results indicate that both functions statistically increased
reliance on AI. Our novel finding is that when radiologists are enabled to control AI output by labeling results
as correct or incorrect, their reliance on AI increases.
1 INTRODUCTION
The integration of artificial intelligence(AI) into med-
ical imaging has revolutionized the field of healthcare,
particularly in areas such as radiology (Lee et al.,
2023) (Sukegawa et al., 2023) (Lew et al., 2024).
These advancements offer new opportunities to en-
hance diagnostic accuracy, improve efficiency, and ul-
timately provide better patient care.
As AI systems continue to demonstrate increas-
ing capabilities in image interpretation, the reliance
rate, which refers to the degree to which medical pro-
fessionals rely on and depend on AI, has become an
important metric for understanding how these tools
are used in practice. The interaction between medical
professionals and AI tools, influenced by the reliance
rate, is now a critical area of study, as it affects both
clinical decision-making and patient outcomes.
a
https://orcid.org/0009-0001-3173-8011
b
https://orcid.org/0000-0002-1454-7512
c
https://orcid.org/0009-0000-1461-5063
d
https://orcid.org/0000-0002-5907-7382
The rapid advancement of deep learning algo-
rithms, particularly in the domain of computer vision,
has also led to the development of AI systems capable
of detecting and classifying a wide range of medical
images with high accuracy.
However, research has shown that people often ex-
hibit low reliance rates on advanced systems, even
when such systems demonstrate superior performance
in certain tasks (Dietvorst et al., 2018) (Logg et al.,
2019). Experts in specific domains tend to exhibit
higher self-efficacy compared with the general people
and are less likely to use advanced systems (Gaube
et al., 2021) (Jussupow et al., 2022) (Nazaretsky et al.,
2022). This suggests that human errors can frequently
occur more with expert than with the general popula-
tion (Filiz et al., 2023) (Meyer et al., 2013).
Our motivation is to adjust the reliance rates of
medical professionals on AI systems to reduce the
likelihood of human errors. By optimizing this re-
liance, we seek to decrease the frequency of diagnos-
tic errors that occur when AI assistance is either un-
derused or ignored.
This paper describes our engineering approach
Miyake, K., Ozaki, K., Maehigashi, A. and Yamada, S.
Adjusting Doctor’s Reliance on AI Through Labeling for Training Data and Modification of AI Output in a Muscle Tissue Detection Task.
DOI: 10.5220/0013187500003890
In Proceedings of the 17th International Conference on Agents and Artificial Intelligence (ICAART 2025) - Volume 3, pages 837-844
ISBN: 978-989-758-737-5; ISSN: 2184-433X
Copyright © 2025 by Paper published under CC license (CC BY-NC-ND 4.0)
837

to adjust medical professionals’, specifically radiolo-
gists and radiographers, reliance on AI systems, with
the ultimate goal of mitigating low reliance and im-
proving overall diagnostic performance.
Therefore, adjusting the reliance rate of medical
professionals on AI systems is crucial for two reasons.
First, it can lead to improved diagnostic accuracy by
combining human experts’ strengths with AI’s com-
putational precision. Second, it can contribute to the
mitigation of human errors that occur due to low re-
liance on AI systems.
On the basis of these considerations, we aimed to
achieve following objectives.
• investigate the effects of AI output modifica-
tion and labeling on radiologists’ and radiogra-
phers’ reliance rates when performing diaphragm-
detection tasks. This objective directly addresses
the need to understand how different forms of in-
teraction with AI systems can influence the radi-
ologists’ and radiographers’ willingness to incor-
porate AI assistance in their diagnostic processes.
• explore how these specific AI interaction func-
tions, modification and labeling, influence radiol-
ogists’ and radiographers’ decision-making pro-
cesses and their perceived utility of AI assistance
in diaphragm detection tasks.
By examining these objectives, we hope to con-
tribute to developing more effective AI integration
strategies to optimize the balance between human ex-
pertise and AI capabilities in clinical settings.
Previous research shows that modifying AI sys-
tems can increase medical professionals’ reliance. We
thus propose to provide the following two functions
for increasing radiologists’ reliance on such systems:
• Labeling AI Outputs. Users can evaluate med-
ical images from AI, and assign labels as correct
or incorrect to prepare training examples for ma-
chine learning.
• Modification AI Outputs. Using a digital pen,
users can directly modify linear segmentation on
a medical image detected by AI.
The remainder of this paper is organized as fol-
lows. Section 2 reviews related work, positioning
our research within the context of literature on AI in
medical imaging and strategies for adjusting reliance
rates. Section 3 details our experiments, data acqui-
sition process, and hypotheses. Section 4 presents
the statistical results, focusing on comparisons be-
tween the experimental conditions. Section 5 pro-
vides a comprehensive discussion of our experimental
results, and Section 6 presents our conclusions.
Figure 1: Touch-screen laptop and stylus used in experi-
ments.
2 RELATED WORK
In this section, we review prior research relevant to
our study, focusing on interface design for AI systems
in medical settings, human responses to algorithmic
forecasts, and factors affecting algorithmic reliance.
We specifically examine how interface simplicity and
user control influence the effectiveness of AI-assisted
decision-making, particularly in medical contexts.
2.1 Factors Influencing Algorithmic
Reliance in Decision-Making
(Mahmud et al., 2022) conducted an extensive sys-
tematic literature review to identify the various factors
influencing reliance on algorithmic decision-making.
They categorized these factors into four main themes:
algorithm-related, individual, task-related, and high-
level. Individual factors, such as age, experience,
and familiarity with algorithms, were found to signif-
icantly influence the degree of reliance.
For instance, older individuals and those with
greater professional experience tend to show lower
reliance on algorithms, preferring their judgment
(Arkes et al., 1986).
Conversely, less experienced individuals are more
likely to rely on algorithmic outputs (Logg et al.,
2019). Psychological traits and perceptions, such as
trust in the algorithm and emotional responses, further
contribute to the variations in reliance rates.
ICAART 2025 - 17th International Conference on Agents and Artificial Intelligence
838

2.2 Impact of User Control on Reliance
on AI
(Dietvorst et al., 2018) investigated the factors that
influence people’s willingness to use imperfect algo-
rithms in decision-making processes. They found that
giving users even the ability to modify an imperfect
algorithm significantly increases their likelihood of
using the algorithm.
(Cheng and Chouldechova, 2023) examined the
impact of user control over algorithm design, compar-
ing the effects of process control (enabling users to af-
fect the input factors or algorithmic models) and out-
come control (enabling users to modify algorithmic
predictions). Their findings highlighted that granting
users the ability to affect the training procedure signif-
icantly increased their likelihood of using the model
and reduced prediction errors.
3 METHODS
3.1 Experimental Environment
The experiment was conducted in a controlled envi-
ronment, with each participant completing tasks in the
same room to ensure consistency in conditions.
The devices used by the participants were HP
Spectre x360 laptops (display resolution 1920×1080
pixels) and the accompanying stylus. The tasks were
performed in tablet mode using the stylus (Figure 2).
This configuration was chosen to provide a consistent
and intuitive interaction method similar to the work-
flow commonly used in clinical settings.
We implemented and conducted the experimen-
tal tasks using jsPsych version 7.2.1. jsPsych is a
JavaScript library for psychology experiments that
enables easy creation and execution of complex be-
havioral experiments in web browsers. The li-
brary’s flexibility enabled us to precisely control the
stimulus-presentation timing and record detailed re-
sponse data. All participants interacted with the
same web-based interface, ensuring standardized con-
ditions across sessions. The experiment was con-
ducted in a Chrome browser to maintain consistency
in the display and response recording.
The medical images used in our experiment were
sourced from the NIH Chest X-ray dataset (Wang
et al., 2017). We randomly selected 40 chest X-ray
images from this dataset regardless of their diagnos-
tic difficulty. The selected images included those with
clear diaphragm boundaries and those with ambigu-
ous boundaries, providing a diverse range of image
characteristics for our evaluation. Under each condi-
tion, one of the images (a total of 4 out of 40) inten-
tionally included incorrect lines drawn by the expert
to simulate errors.
3.2 Participants
Before collecting data, we conducted a priori power
analysis using G*Power 3.1 (Faul et al., 2007) to de-
termine the required sample size for our two-way re-
peated measures analysis of variance(ANOVA). The
analysis was based on the following parameters: an
effect size of 0.25, significance level of 5%, and
power of 80%. The required sample size was calcu-
lated to be 24 cases.
To control for the order effects under the exper-
imental conditions, we used a counterbalanced de-
sign. After the initial 10 baseline trials, the remain-
ing 30 trials were presented in a randomized order
across the 3 experimental conditions (modification,
labeling, and combined). This randomization was im-
plemented to minimize potential carryover effects be-
tween conditions and to control for fatigue or learn-
ing effects that might occur during the experiment. A
total of 25 radiologists and radiographers with rele-
vant experience in medical imaging (19 males, 6 fe-
males; age range: 24–54 years, median = 29; years
of experience: 0-30 years, median = 3) participated
in the experiment. The participants were recruited
from staff members of Hamamatsu University School
of Medicine Hospital. Data from all participants were
included in the analysis, with no exclusions. Partici-
pants received 2,000 yen (approximately 13 USD) for
completing half an hour of the experiment.
3.3 Experimental Design
The experiments involved a 2×2 within-participants
design to evaluate the effectiveness of two distinct
AI-interaction factors, i.e., labeling and modification.
Each factor had two levels (enable vs. disable), re-
sulting in four experimental conditions:
1. Control Condition. If participants chose the AI,
they were unable to view the AI output and dele-
gated the task entirely to the AI.
2. Labeling Condition. If participants chose the AI,
they were able to label the AI output as correct or
incorrect.
3. Modification Condition. If participants chose
the AI, they were able to modify the AI output.
However, if they thought the output was appropri-
ate, they could leave it unchanged.
Adjusting Doctor’s Reliance on AI Through Labeling for Training Data and Modification of AI Output in a Muscle Tissue Detection Task
839
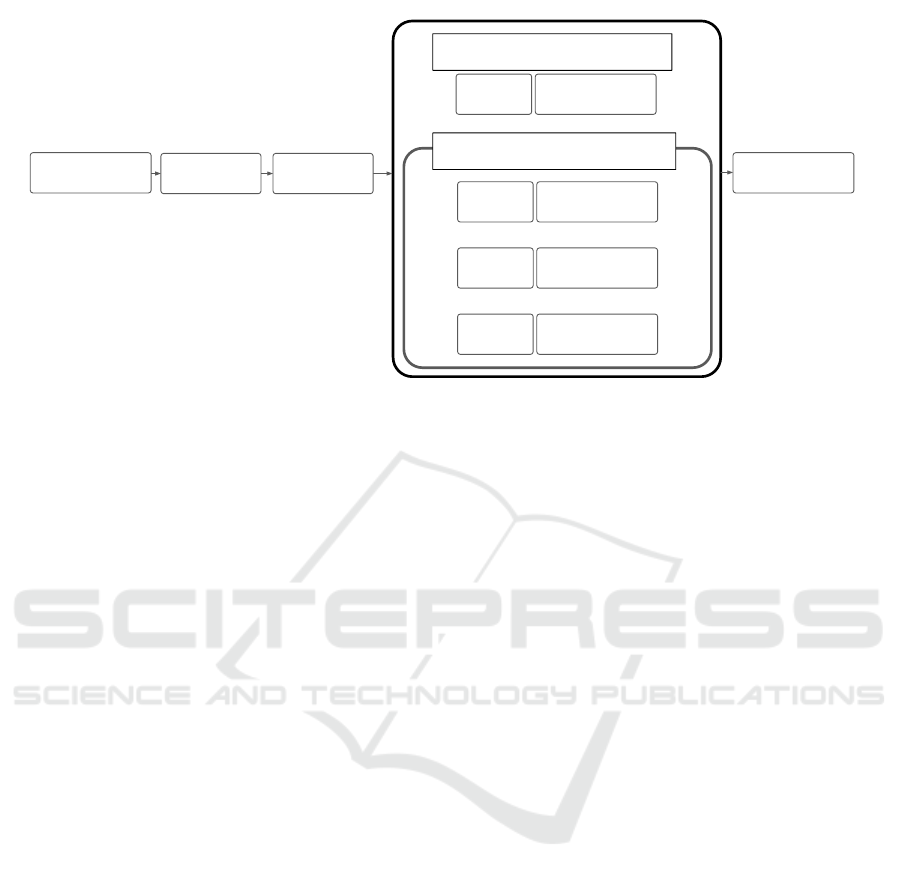
Pre-
Questionnaire
2nd-4th Conditions (random)
1st Condition
10 trials under each conditions
Experiment
Explanation
Modification
Practice
×Modification
×Labeling
AI or Self
〇Modification
×Labeling
AI or Self
×Modification
〇Labeling
AI or Self
〇Modification
〇Labeling
AI or Self
Post-
Questionnaire
Figure 2: Overall flow of experiment.
4. Combined Condition. If participants chose the
AI, they were able to label the AI output as correct
or incorrect. If they labeled it as incorrect, they
were able to modify the AI output.
3.4 Diaphragm-Detection Task
The task involved diaphragm detection on chest X-
ray images (two-images are shown on the display
in Figure 1). Participants were asked to detect and
draw lines on diaphragm outlines on the image using
a stylus interface. Specifically, participants were in-
structed to draw lines along the diaphragm boundaries
using two colors: red for the right diaphragm and blue
for the left diaphragm.
For each task trial, participants viewed an X-ray
image display on a vertically oriented screen and used
a stylus pen to draw the outlines. The interface en-
abled participants to draw precise lines and make cor-
rections as needed. The interface also provided edit-
ing capabilities through undo, redo, and clear buttons.
3.5 Hypotheses
On the basis of the literature and identified research
gap, we propose the following hypotheses:
H1. The function to label AI output increases the rate
of AI utilization among medical professionals.
H2. The function to modify AI output increases the
rate of AI utilization among medical profession-
als.
The first hypothesis is grounded in previous re-
search in a different domain from the medical domain.
Studies have shown that giving users some control
over algorithmic processes can increase their willing-
ness to use AI systems (Dietvorst et al., 2018). By ex-
tending this concept to the medical imaging domain,
we aimed to test specific forms of user interaction.
The second hypothesis is motivated by the poten-
tial of user feedback to enhance the perceived reli-
ability of AI systems. The act of labeling may en-
gage medical professionals in a more critical evalu-
ation of AI output, promote a sense of collaboration
rather than replacement, and potentially increase their
willingness to rely on AI assistance.
3.6 Procedure
Figure 2 provides an overview of the experimen-
tal process. Our experiment started with a pre-
questionnaire that participants completed to gather
demographic information and assess their experience
with and attitudes toward AI in medical settings. The
questionnaire collected data on participants’ gender,
age, and years of professional experience in the cur-
rent position.
After the pre-questionnaire, participants were in-
formed that the AI system was trained on data from
a radiologist with over 20 years of experience. This
information was provided to establish the perceived
reliability and expertise of the AI system.
However, these AI outputs were directly made by
the radiologist with over 20 years of experience, not
generated by AI. The expert radiologist used a stylus
to draw lines directly on the medical images. These
pre-annotated images were presented to the partici-
pants as AI outputs.
Participants were then instructed to perform a task
involving drawing red lines on the right diaphragm
ICAART 2025 - 17th International Conference on Agents and Artificial Intelligence
840
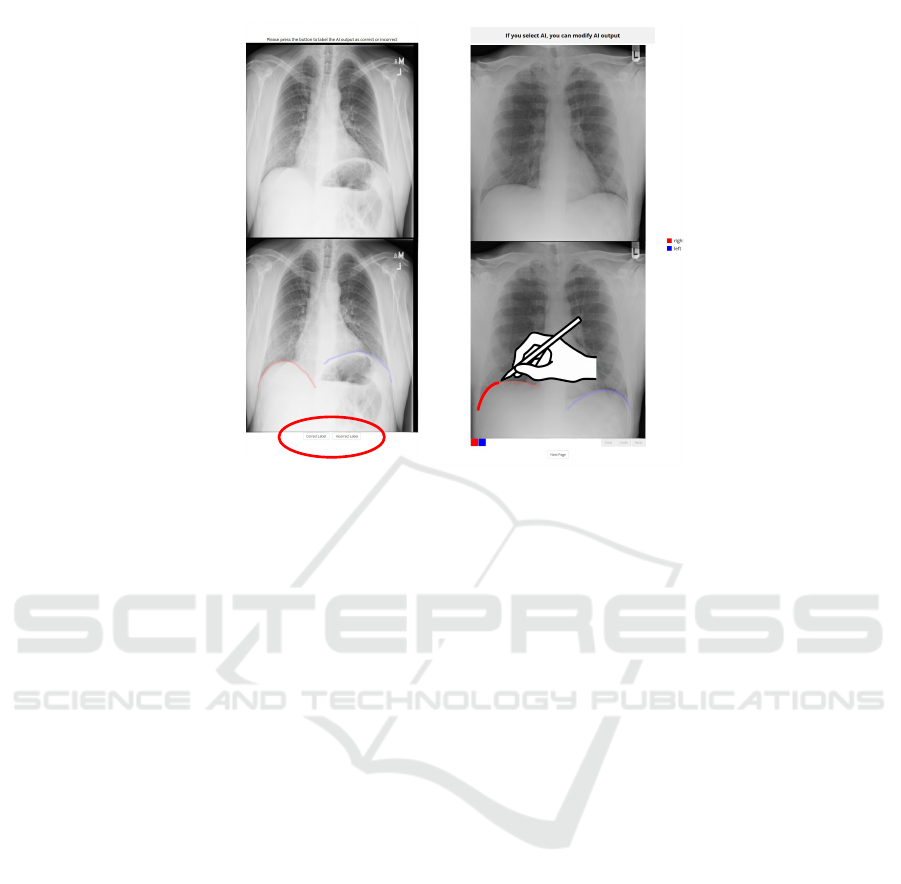
Labeling Condition
Modification Condition
Figure 3: Task process of labeling and modification conditions.
and blue lines on the left diaphragm. For each task,
they were given the option to either use AI assistance
or draw the lines themselves, regardless of the exper-
imental condition. Participants were also informed
that when they chose to use AI, the specific opera-
tions they could perform with the AI output would be
displayed above the original image. This information
was provided to ensure participants understood what
they could do and the interface for each trial.
The screen was then oriented vertically, and par-
ticipants transitioned to using a stylus for input. They
completed a single practice session to modify an AI
output. This practice was designed to help partici-
pants become familiar with the use of the stylus and
touchscreen interface, ensuring they would be com-
fortable with the interaction function during the main
tasks.
Following the practice session, the experiment
proceeded in two phases:
• Initial Reliance Rate Assessment: Participants
completed ten trials with no modification and no
labeling to establish an initial reliance rate.
• Main Experimental Conditions: Participants un-
derwent 30 trials, with each trial randomly as-
signed to one of 3 experimental conditions: modi-
fication, labeling, or combined (both modification
and labeling).
For all four conditions, each trial began with par-
ticipants choosing whether to use AI or perform the
task themselves. The subsequent procedure varied on
the basis of this choice and the conditions (Figure 3):
1. Control Condition:
• If AI Was Selected. A message indicated
that the task was delegated to AI, and the trial
ended.
• If Self-Selected. The original X-ray image was
presented for the participant to draw lines.
2. Modification Condition:
• If AI Was Selected. Two images were pre-
sented, the original X-ray image (top) and the
image drawn by the AI (bottom). Participants
could modify the AI output or proceed without
changes if they agreed with the AI.
• If Self-Selected. Same as the control condition
3. Labeling Condition:
• If AI Was Selected. Two images were pre-
sented as in the modification condition. Partic-
ipants labeled the AI output as correct or incor-
rect using buttons at the bottom of the screen.
• If Self-Selected. Same as the control condition.
4. Combined Condition:
• If AI Was Selected. Participants first labeled
the AI output as in the labeling condition. If
labeled as incorrect, they could modify the AI
output as in the modification condition.
• If Self-Selected. Same as the control condition.
After completing all 40 trials, participants were
asked to complete a post-questionnaire.
Adjusting Doctor’s Reliance on AI Through Labeling for Training Data and Modification of AI Output in a Muscle Tissue Detection Task
841

** **
Conditions
Mod&Label Mod Label
Choice-only
Reliance Rate [%]
100
75
50
25
0
** : <.01
Figure 4: Box plot of reliance rates for all four conditions.
Plot illustrates distribution of reliance rates under different
combinations of modification and labeling functions.
4 RESULTS
We conducted a 2 (Modification: enable to modify
vs. disable to modify) × 2 (Labeling: enable to la-
bel vs. disable to label) repeated measures ANOVA
on reliance rate as a dependent variable. This anal-
ysis enabled us to examine the individual and com-
bined effects of modification and labeling capabilities
on participants’ reliance on AI assistance in the task.
Figure 4 shows that the ANOVA revealed a sig-
nificant main effects for both the modification factor
(F(1, 24) = 19.25, p < .001, partial 𝜂
2
= 0.45), and la-
beling factor (F(1, 24) = 24.22, p < .001, partial 𝜂
2
=
0.50), as well as a significant interaction effect (F(1,
24) = 19.39, p < .001, partial 𝜂
2
= 0.45).
To further examine these effects, we investigated
a simple main effect analysis using Holm’s correc-
tion (Table 1). The results indicated significant simple
main effects of the labeling factor under the modifica-
tion factor (F(1, 24) = 27.24, 𝑝
ℎ𝑜𝑙𝑚
< .000, partial 𝜂
2
= 0.00), and of the modification factor under the la-
beling factor (F(1, 24) = 21.19, 𝑝
ℎ𝑜𝑙𝑚
< .000, partial
𝜂
2
= 0.08).
5 DISCUSSION
We aimed to investigate the influence of modifica-
tion and labeling capabilities on medical profession-
als’, specifically radiologists and radiographers, re-
liance on AI systems in image interpretation tasks.
The results provide insights into adjusting reliance
rates in medical situations. We observed the effects
of both modification and labeling capabilities on re-
liance rates.
5.1 Hypotheses Summary
The results of our statistical analyses provide support
for both hypotheses.
The first hypothesis is that the function to mod-
ify AI output will increase the rate of AI utilization
among medical professionals. This hypothesis was
supported by our analysis, which revealed a statis-
tically significant increase in the reliance rate when
participants were able to modify AI output compared
with the control condition. This finding suggests that
enabling users to modify AI output effectively en-
courages them to do so.
The second hypothesis proposed that the function
to label AI output will increase the rate of AI utiliza-
tion among medical professionals. This hypothesis
was also supported. The data indicates a statistically
significant increase in reliance rates when participants
were able to label AI output as correct or incorrect,
compared with the control condition. This indicates
that the act of labeling AI output contributes to in-
creasing acceptance and use of AI assistance.
5.2 Two Functions Effect on Reliance
Rate
The function to modify AI outputs demonstrated a
significant effect on reliance rates. These findings
align with previous research by Dietvorst et al., who
found that giving users even a small amount of mod-
ification for an imperfect algorithm significantly in-
creases their likelihood of using it. In our medical
context, the option to modify AI output likely pro-
vided participants with a sense of control over the
decision. This control may have mitigated concerns
about the AI system’s potential errors or biases, lead-
ing to increased reliance.
The labeling functions, which enabled partici-
pants to categorize AI outputs as correct or incorrect,
also significantly affected reliance rates. This find-
ing introduces a novel perspective to the literature on
human-AI interaction. The act of labeling may have
several beneficial effects on user perception and be-
havior. Labeling encourages active engagement with
AI output, prompting users to critically evaluate the
system’s performance. This increased engagement
may lead to a better understanding of AI capabilities
and limitations.
5.3 Limitation and Future Work
Though we experimentally confirmed the effective-
ness of two functions to increase reliance rate, limi-
tations should be noted. The study was conducted in
ICAART 2025 - 17th International Conference on Agents and Artificial Intelligence
842
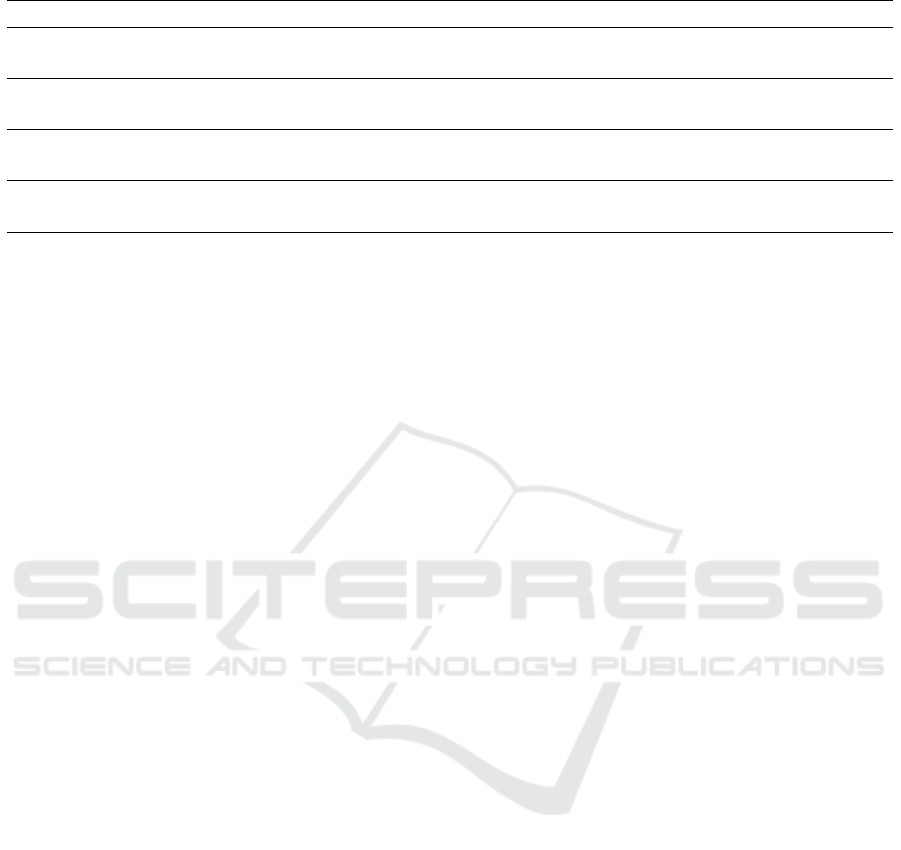
Table 1: Results of simple main effects for reliance rates across conditions.
Conditions Sum of Squares df Mean Square 𝐹 𝑝 𝜂
2
𝑝
Mod * Label - Label 128.00 1 128.00 1.95 0.18 0.08 n.s.
1572.00 24 65.50
Mod - Control 12800.00 1 12800.00 21.19 0.00 0.47 ∗∗
𝑎
14500.00 24 604.17
Mod * Label - Label 8.00 1 8.00 0.08 0.78 0.00 n.s.
2492.00 24 103.83
Label - Control 10952.00 1 10952.00 27.24 0.00 0.53 ∗∗
𝑎
9648.00 24 402.00
𝑎
** indicates p < .01.
a controlled environment focusing on a specific mus-
cle tissue detection task. Future research should ex-
plore these effects in diverse clinical settings, across
various medical specialties, and over longer periods
to understand their impact on reliance rates.
This study also focused on the increase in reliance
rates, but it is important to consider this in different
environments, there is a potential risk of over-reliance
on AI systems (Cecil et al., 2024) (Klingbeil et al.,
2024). This could lead to inappropriate decision-
making if AI advice is followed uncritically. Conse-
quently, further investigations should aim to examine
methods for balancing appropriate reliance with miti-
gating the risk of over-reliance, ensuring that AI sys-
tems are integrated effectively without compromising
human judgment.
Another critical limitation is concerned to respon-
sibility. Since AI systems cannot take responsibility
for decisions, fully relying on AI in clinical practice
remains challenging. The lack of clear responsibility
and accountability in AI systems means that human
oversight will continue to be necessary, and this may
affect the degree to which healthcare professionals are
willing to rely on AI.
Due to the nature of the task, which involved
drawing lines to mark specific areas, it was challeng-
ing to determine clear right or wrong answers. It
was therefore difficult to compare performance out-
comes between different conditions. This limitation
highlights the need for further studies that incorporate
more objective performance metrics to fully evaluate
the impact of interaction design on user effectiveness.
Another avenue for future research involves ex-
amining the interaction between the attribution of re-
sponsibility to data providers or holders and the au-
thority of supervising clinicians. Investigating these
dynamics could offer new insights into how different
accountability structures influence reliance on AI sys-
tems in healthcare settings. Understanding this inter-
action could help address concerns about both under-
reliance and over-reliance, ensuring that AI is used as
a supportive tool rather than an unquestioned author-
ity.
6 CONCLUSIONS
We examined how modification and labeling of AI
outputs affect medical professionals’ reliance on AI
systems in diaphragm detection tasks. Our findings
indicate that both functions can significantly increase
reliance rates.
The function to modify AI outputs and label them
as correct or incorrect appeared to increase user re-
liance, potentially by providing a sense of control and
encouraging critical evaluation. These results have
important implications for the design of AI systems
in medical settings, suggesting that incorporating the
interactive functions may optimize reliance rates and
improve AI integration in clinical practice. Our study
will contribute to the growing research on human-AI
interaction in healthcare, offering insights into how
interaction design influences user behavior.
As AI systems become increasingly prevalent in
clinical settings, optimizing human-AI interaction re-
mains crucial. While our findings suggest promis-
ing avenues for improving AI integration in medi-
cal image interpretation, the complexity of balancing
increased reliance with appropriate human oversight
also remains to be explored. Continued research in
this area is essential to ensure that AI tools enhance
the quality of patient care.
ACKNOWLEDGEMENTS
This work was partially supported by JST, CREST
(JPMJCR21D4), Japan.
Adjusting Doctor’s Reliance on AI Through Labeling for Training Data and Modification of AI Output in a Muscle Tissue Detection Task
843

REFERENCES
Arkes, H. R., Dawes, R. M., and Christensen, C. (1986).
Factors influencing the use of a decision rule in a prob-
abilistic task. Organizational Behavior and Human
Decision Processes, 37(1):93–110.
Cecil, J., Lermer, E., Hudecek, M. F. C., Sauer, J., and
Gaube, S. (2024). Explainability does not mitigate the
negative impact of incorrect AI advice in a personnel
selection task. Scientific Reports, 14(1):1–15.
Cheng, L. and Chouldechova, A. (2023). Overcoming algo-
rithm aversion: A comparison between process and
outcome control. In Proceedings of the 2023 CHI
Conference on Human Factors in Computing Systems,
number Article 756 in CHI ’23, pages 1–27.
Dietvorst, B. J., Simmons, J. P., and Massey, C. (2018).
Overcoming algorithm aversion: People will use im-
perfect algorithms if they can (even slightly) modify
them. Management Science, 64(3):1155–1170.
Faul, F., Erdfelder, E., Lang, A.-G., and Buchner, A. (2007).
G*Power 3: a flexible statistical power analysis pro-
gram for the social, behavioral, and biomedical sci-
ences. Behavior Research Methods, 39(2):175–191.
Filiz, I., Judek, J. R., Lorenz, M., and Spiwoks, M.
(2023). The extent of algorithm aversion in decision-
making situations with varying gravity. PLOS One,
18(2):e0278751.
Gaube, S., Suresh, H., Raue, M., Merritt, A., Berkowitz,
S. J., Lermer, E., Coughlin, J. F., Guttag, J. V., Colak,
E., and Ghassemi, M. (2021). Do as AI say: suscep-
tibility in deployment of clinical decision-aids. NPJ
Digit Medcine, 4(1):31.
Jussupow, E., Spohrer, K., and Heinzl, A. (2022). Radiol-
ogists’ usage of diagnostic AI systems. Business &
Information Systems Engineering, 64(3):293–309.
Klingbeil, A., Gr
¨
utzner, C., and Schreck, P. (2024). Trust
and reliance on AI — an experimental study on the
extent and costs of overreliance on AI. Computers in
Human Behavior, 160:108352.
Lee, J. H., Hong, H., Nam, G., Hwang, E. J., and Park,
C. M. (2023). Effect of human-AI interaction on
detection of malignant lung nodules on chest radio-
graphs. Radiology, 307(5):e222976.
Lew, C. O., Calabrese, E., Chen, J. V., Tang, F., Chaudhari,
G., Lee, A., Faro, J., Juul, S., Mathur, A., McKinstry,
R. C., Wisnowski, J. L., Rauschecker, A., Wu, Y. W.,
and Li, Y. (2024). Artificial intelligence outcome pre-
diction in neonates with encephalopathy (AI-OPiNE).
Radiology: Artificial Intelligence, page e240076.
Logg, J. M., Minson, J. A., and Moore, D. A. (2019). Algo-
rithm appreciation: People prefer algorithmic to hu-
man judgment. Organizational Behavior and Human
Decision Processes, 151:90–103.
Mahmud, H., Islam, A. K. M. N., Ahmed, S. I., and
Smolander, K. (2022). What influences algorithmic
decision-making? a systematic literature review on al-
gorithm aversion. Technological Forecasting and So-
cial Change, 175:121390.
Meyer, A. N. D., Payne, V. L., Meeks, D. W., Rao, R., and
Singh, H. (2013). Physicians’ diagnostic accuracy,
confidence, and resource requests: A vignette study.
JAMA Internal Medicine, 173(21):1952–1958.
Nazaretsky, T., Ariely, M., Cukurova, M., and Alexandron,
G. (2022). Teachers’ trust in AI -powered educational
technology and a professional development program
to improve it. British Journal of Educational Technol-
ogy, 53(4):914–931.
Sukegawa, S., Ono, S., Tanaka, F., Inoue, Y., Hara, T.,
Yoshii, K., Nakano, K., Takabatake, K., Kawai,
H., Katsumitsu, S., Nakai, F., Nakai, Y., Miyazaki,
R., Murakami, S., Nagatsuka, H., and Miyake, M.
(2023). Effectiveness of deep learning classifiers in
histopathological diagnosis of oral squamous cell car-
cinoma by pathologists. Scientific Reports, 13(1):1–9.
Wang, X., Peng, Y., Lu, L., Lu, Z., Bagheri, M., and Sum-
mers, R. M. (2017). ChestX-Ray8: Hospital-scale
chest X-ray database and benchmarks on weakly-
supervised classification and localization of common
thorax diseases. In Proceedings of the 2017 IEEE
Conference on Computer Vision and Pattern Recog-
nition, pages 3462–3471. IEEE.
ICAART 2025 - 17th International Conference on Agents and Artificial Intelligence
844
