
Integrating Clinical Expertise into Software Development: Evaluating
the Use of openEHR Archetypes for Requirements Elicitation in
Healthcare Applications
Jos
´
e Silva
a
and Andr
´
e Ara
´
ujo
b
Computing Institute, Federal University of Alagoas, Av. Lourival Melo Mota, S/N - Cidade Universit
´
aria, Macei
´
o, Brazil
Keywords:
OpenEHR Archetypes, Software Requirements Elicitation, Healthcare Professionals.
Abstract:
OpenEHR archetypes are standardized frameworks designed to model clinical information in healthcare sys-
tems, enabling a consistent and integrated representation of complex data. These models encompass common
clinical elements such as symptoms, diagnoses, and treatments, ensuring that information is understood and
applied uniformly across different contexts. This paper investigates the use of openEHR archetypes in the
requirements elicitation and specification process for clinical systems, highlighting their potential to integrate
healthcare professionals’ knowledge into software development. The literature review reveals a significant
gap in the participation of these professionals during the requirements elicitation phase, especially in studies
that apply archetypes. Quantitative and qualitative results positively perceive the methodology used, high-
lighting clarity, collaboration, and alignment with end-user needs. Statistical analysis using the Wilcoxon test
presented significant p-values, indicating that professionals considered the method straightforward, intuitive,
and conducive to engagement, with real opportunities for contribution to the validation of requirements. The
qualitative data reinforce the importance of a collaborative environment and suggest the need for deeper in-
volvement of healthcare professionals at all process stages. In conclusion, this research indicates that applying
openEHR archetypes, combined with more significant interaction with healthcare professionals, is promising
for integrating clinical expertise effectively and directly into developing clinical systems.
1 INTRODUCTION
The health sector is vital to society, influencing indi-
viduals’ quality of life and well-being. With grow-
ing population demands and complex care needs, de-
veloping efficient, accessible healthcare applications
is a priority (Bitkina et al., 2020). Active participa-
tion from healthcare professionals throughout devel-
opment ensures systems address specific needs, prior-
itizing usability, security, and accuracy while reflect-
ing clinical practices (Barbosa et al., 2021; Maramba
et al., 2019).
The openEHR archetype standard supports inter-
operability and standardization of healthcare data,
structuring clinical information consistently across
platforms (Badr, 2019; de Ara
´
ujo et al., 2016). Each
archetype represents a clinical concept, such as di-
agnosis or medication, organizing data in a reusable
and extensible way. Academically, openEHR
a
https://orcid.org/0009-0001-0225-2696
b
https://orcid.org/0000-0001-8321-2268
archetypes are studied for improving health data qual-
ity and modeling requirements in complex systems
(de Ara
´
ujo et al., 2019; Chen et al., 2009). In indus-
try, they are used to build interoperable applications
that integrate data and support patient care continuity
(Ding et al., 2023). Their adoption highlights their po-
tential as a robust standard for safe, effective clinical
applications (Ferreira and de Souza, 2023).
End-user involvement is critical in software de-
velopment to ensure requirements reflect the prob-
lem domain, particularly in healthcare, where clini-
cal knowledge impacts patient safety (Govella, 2019).
Engaging healthcare professionals during require-
ments elicitation ensures solutions align with clini-
cal realities (Leslie, 2020; Tian et al., 2021; Hak
et al., 2020; Silva et al., 2024). While openEHR
archetypes are traditionally used for EHR standard-
ization and interoperability during development (Li
et al., 2021; Wulff et al., 2021; Arevshatyan et al.,
2020), their application in elicitation could formalize
specialist knowledge earlier, optimizing development.
This research explores whether using openEHR
672
Silva, J. and Araújo, A.
Integrating Clinical Expertise into Software Development: Evaluating the Use of openEHR Archetypes for Requirements Elicitation in Healthcare Applications.
DOI: 10.5220/0013226900003911
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 18th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2025) - Volume 2: HEALTHINF, pages 672-679
ISBN: 978-989-758-731-3; ISSN: 2184-4305
Proceedings Copyright © 2025 by SCITEPRESS – Science and Technology Publications, Lda.

archetypes in requirements elicitation aids in identify-
ing and expressing domain expert knowledge during
healthcare application development. We examine if
archetypes can effectively capture clinical needs, en-
hancing communication between developers and spe-
cialists while ensuring that the solutions align with
healthcare professionals’ requirements.
We conducted interviews and practical activities
with openEHR archetypes involving healthcare pro-
fessionals to evaluate their role in bridging commu-
nication gaps and accurately representing clinical re-
quirements.
The article is organized as follows: Section 2 in-
troduces openEHR archetypes, their structure, and
applications. Section 3 details the study methodol-
ogy. Section 4 analyzes related work on archetypes in
health systems. Section 5 presents our study, method-
ology, and insights. Section 6 concludes with remarks
and future research directions on archetypes in health-
care software development.
2 OpenEHR ARCHETYPE
An archetype is a reusable, structured model that de-
fines clinical concepts and data structures necessary
for capturing healthcare information (Palojoki et al.,
2024; da Silva et al., 2019). These archetypes rely on
two core models: the reference and archetype mod-
els (openEHR Foundation, 2024b). The reference
model provides foundational structure and data types
for interoperability, representing entities, attributes,
and relationships consistently in health systems. The
archetype model outlines specific clinical content
within the reference model, such as diagnoses, treat-
ments, and measurements. This dual modeling ap-
proach separates clinical knowledge from techni-
cal constraints, facilitating adaptation and mainte-
nance of clinical information across health applica-
tions (openEHR Foundation, 2024a).
Archetypes include key elements that enhance
adaptability for clinical scenarios (Ferreira and
de Souza, 2023). Primary components are data at-
tributes, terminologies, and constraints. Data at-
tributes capture specific clinical data, such as patient
identifiers or observations. Terminologies ensure con-
sistent use of clinical vocabularies, linking data to
standardized medical coding systems. Constraints
limit values or structures, maintaining data quality
and consistency across implementations.
Templates combine multiple archetypes into
structured forms tailored to clinical workflows (Badr,
2019). These templates customize archetypes for
specific use cases, offering flexibility in their appli-
cation. The Clinical Knowledge Manager (CKM)
serves as a repository for openEHR archetypes and
templates, enabling access, sharing, and collabora-
tion among healthcare professionals and developers
(Foundation, 2023). CKM promotes reuse of stan-
dardized archetypes, ensuring consistency and inter-
operability in healthcare data models.
The Archetype Editor is a tool for creating and
specifying openEHR archetypes (Moner et al., 2018).
It enables users to define, edit, and validate archetypes
by structuring clinical concepts with data attributes,
terminologies, and constraints. This tool facilitates
precise modeling of clinical concepts, improving in-
teroperability and data accuracy. Users can specify
elements such as data attributes, permissible values,
terminology bindings, and constraints, ensuring struc-
tured clinical models align with the dual-model ap-
proach.
The tool supports collaborative development, in-
corporating clinician feedback to ensure relevance. It
plays a key role in the openEHR ecosystem, enabling
standardized archetypes for integration into templates
and repositories like CKM. Figure 1 illustrates an
archetype specified in the Archetype Editor, show-
ing organized sections for data attributes, terminology
bindings, and constraints, which ensure data consis-
tency and quality.
3 METHODOLOGY
This section describes the ethical considerations
and methodological approach that guided this study.
Firstly, institutional and legal regulations describe the
ethical aspects guaranteeing participants’ protection
and privacy. Finally, the methodological path is pre-
sented, explaining the stages of reviewing literature
and conducting the practical study with health profes-
sionals using archetypes.
3.1 Ethical Considerations
The research followed the ethical principles estab-
lished by the Brazilian resolution, considering the es-
sential pillars of bioethics and human rights. It was
ensured that all participants received precise informa-
tion about the objectives and methods of the research,
with emphasis on the voluntary nature of participation
and the protection of anonymity and confidentiality of
data.
Interactions with the participants only took place
after they had signed the Informed Consent Form
(ICF). The data processing and confidentiality strate-
gies were detailed, guaranteeing the security of per-
Integrating Clinical Expertise into Software Development: Evaluating the Use of openEHR Archetypes for Requirements Elicitation in
Healthcare Applications
673
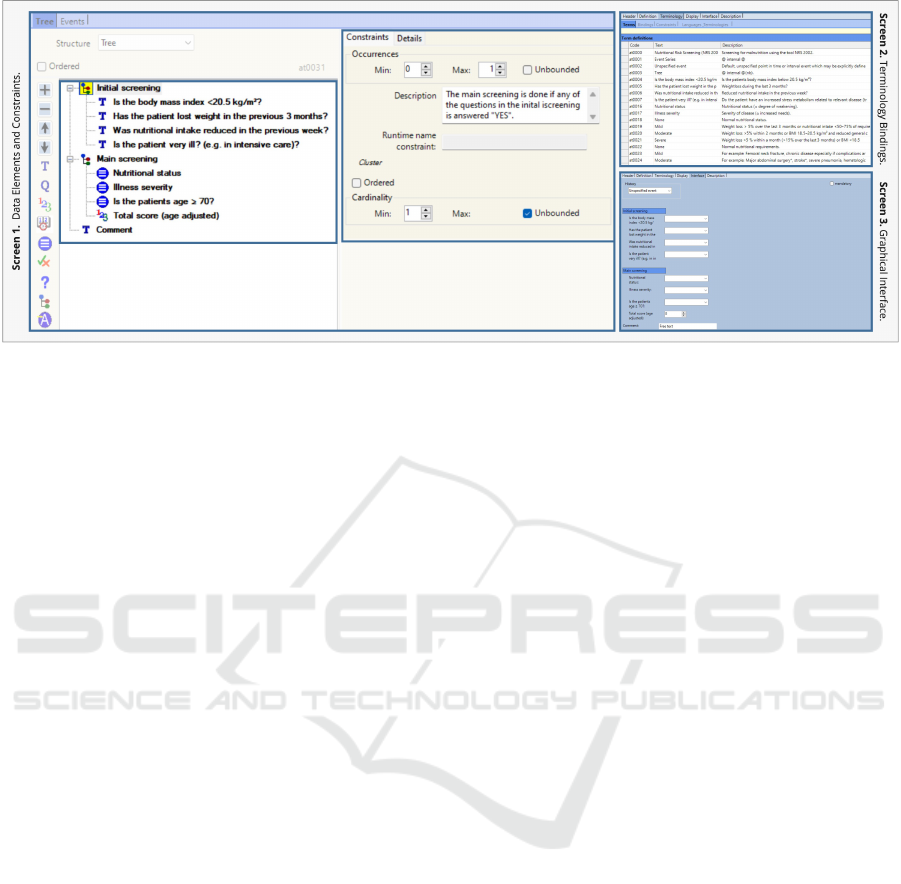
Figure 1: Representation of the elements of an archetype.
sonal data and sensitive information that might arise
during the interviews and questionnaires.
3.2 Methodological Approach
The research methodology consisted of a literature re-
view and a practical study using archetypes, as shown
in Figure 2. The literature review aimed to analyze
studies using archetypes in healthcare software devel-
opment. This involved reviewing ten studies, synthe-
sizing findings, and discussing them to contextualize
the research proposal. Based on this synthesis, the
research question for the practical study was formu-
lated.
In the practical study, archetypes were used to
simulate a patient anamnesis and follow-up scenario
with fourteen healthcare professionals. This aimed
to demonstrate and specify requirements, collecting
both qualitative and quantitative data. The study
explored professionals’ perceptions of archetypes in
software requirements elicitation for healthcare. Af-
ter the interviews, a structured form with three Likert-
scale questions was administered to capture partic-
ipants’ perceptions. The collected data underwent
qualitative and statistical analyses, and the results
were discussed in the final stage of the study.
4 RELATED WORK
The related work section is divided into two main
parts: a state-of-the-art analysis and a discussion.
In the state-of-the-art analysis, we review existing
studies on using openEHR archetypes, focusing on
their objectives, methodologies, and findings in de-
tail. This analysis thoroughly overviews current ap-
proaches and trends in applying openEHR archetypes
in healthcare. Following this, the discussion synthe-
sizes the insights gained from the study, highlighting
gaps, limitations, and potential areas for further re-
search.
4.1 State of the Art Analysis
In healthcare, clinical data modeling has advanced to
better meet the needs and expertise of healthcare pro-
fessionals. In this context, openEHR archetypes stan-
dardize health data and incorporate specific insights
and knowledge provided by professionals at various
stages of application development. Thus, this section
analyzes related works to investigate how each study
employs openEHR archetypes, including the level of
involvement of healthcare professionals, based on the
observations in Table 1.
In the context of clinical standardization, the study
(Tian et al., 2021) focused on automating the cre-
ation of data quality rules in a Chinese hospital, using
archetypes to ensure data consistency and complete-
ness. Meanwhile, the study by (Oliveira et al., 2022)
explored the use of archetypes to standardize requests
for complementary diagnostics, enabling the creation
of indicators to monitor waiting times and test execu-
tion. However, neither of the studies specified when
the archetypes were modeled, at which phase they
were applied nor did they involve end users directly.
The study by (Wulff et al., 2021) aimed to stan-
dardize microbiological data for infection control, us-
ing archetypes to create a reusable model for different
institutions. In contrast to the studies in (Tian et al.,
2021) and (Oliveira et al., 2022), (Wulff et al., 2021)
actively involved healthcare professionals during the
development and validation phases, which was essen-
tial to ensure the proposed model’s applicability in
real-world scenarios.
HEALTHINF 2025 - 18th International Conference on Health Informatics
674
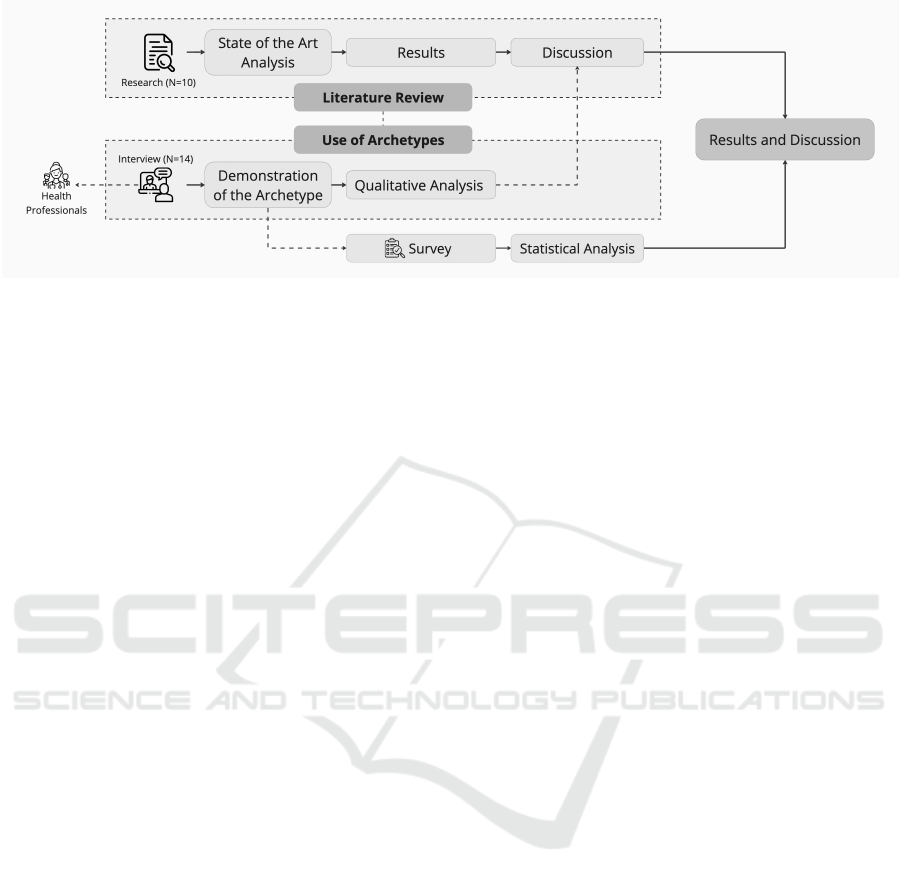
Figure 2: Methodological Approach.
Regarding screening and monitoring, the study (Li
et al., 2020) developed a shared model for COVID-19
based on Chinese guidelines, applying archetypes to
model clinical data, but without specifying at which
stage of the development cycle this was used. This
work did not involve direct interaction with healthcare
professionals. Similarly, the study (Li et al., 2022)
proposed a methodology to measure clinical quality,
integrating openEHR with Clinical Quality Language
(CQL) in the application development phases, involv-
ing doctors directly to provide feedback and adjust
quality indicators, improving the system’s usability.
In the context of clinical decision support, the
study (Silva et al., 2023) focused on rehabilitation
medicine and sought to develop a platform for collect-
ing and consolidating clinical data using archetypes
during the elicitation and development phases. In
this study, healthcare professionals did not partici-
pate in archetype modeling but were involved in re-
quirements gathering, which was critical for structur-
ing the platform’s standardized data. The study (Hak
et al., 2020) discusses the adoption of the openEHR
standard with a focus on health information manage-
ment. In this case, archetypes were applied during
validation phases, with engineers and clinical pro-
fessionals working together to ensure the platform’s
usability and its impact on clinical practice. The
study (Li et al., 2021) developed an openEHR-based
screening tool for strokes, applying archetypes during
both development and validation phases for eligibility
queries in electronic health records (EHRs). The tool
was refined with input from healthcare professionals
to enhance its accuracy and clinical applicability in
medical consultations.
Finally, in the category of clinical use of EHRs,
the study (Leslie, 2020) explored the reuse of
openEHR archetypes in multilingual COVID-19 clin-
ical data, focusing on symptom tracking. Archetypes
were applied without the direct participation of end
users, as the development followed international clin-
ical guidelines. Similarly, (Arevshatyan et al., 2020)
focused on the integration of clinical and genomic
data for cancer treatment in two hospitals in Paraguay,
applying archetypes during the development and val-
idation phases, involving oncologists in the process,
and ensuring the system met the needs of oncological
data analysis.
4.2 Discussion
The analysis of the ten papers listed in Table 1 reveals
that all the articles utilize openEHR archetypes in de-
veloping their healthcare applications. This approach
aims to create standardized, interoperable solutions
suitable for clinical contexts. Healthcare profession-
als are recognized as the end users for all the appli-
cations, highlighting that these tools are designed to
support their practical activities. However, only six
of the ten papers involve healthcare professionals at
some point during the development process, primar-
ily for validation purposes, and they do not participate
directly in the initial stages.
A standard limitation in the studies is the lack of
involvement from healthcare professionals during the
elicitation and prototyping phases of archetype mod-
eling. This suggests that clinical requirements are
often defined based on external guidelines or tech-
nical knowledge rather than through active collabo-
ration with the professionals who will use the appli-
cations. Additionally, five studies do not specify at
which stage of development archetype modeling oc-
curs, making it challenging to understand how the
needs of end users have been translated into techno-
logical solutions.
In addition, the studies analyzed are distributed in
four focus areas: clinical standardization, screening
and monitoring, clinical decision support, and clini-
cal use of EHRs. Each of these areas addresses spe-
cific aspects of the needs of healthcare professionals;
however, the lack of interaction in the early stages
Integrating Clinical Expertise into Software Development: Evaluating the Use of openEHR Archetypes for Requirements Elicitation in
Healthcare Applications
675
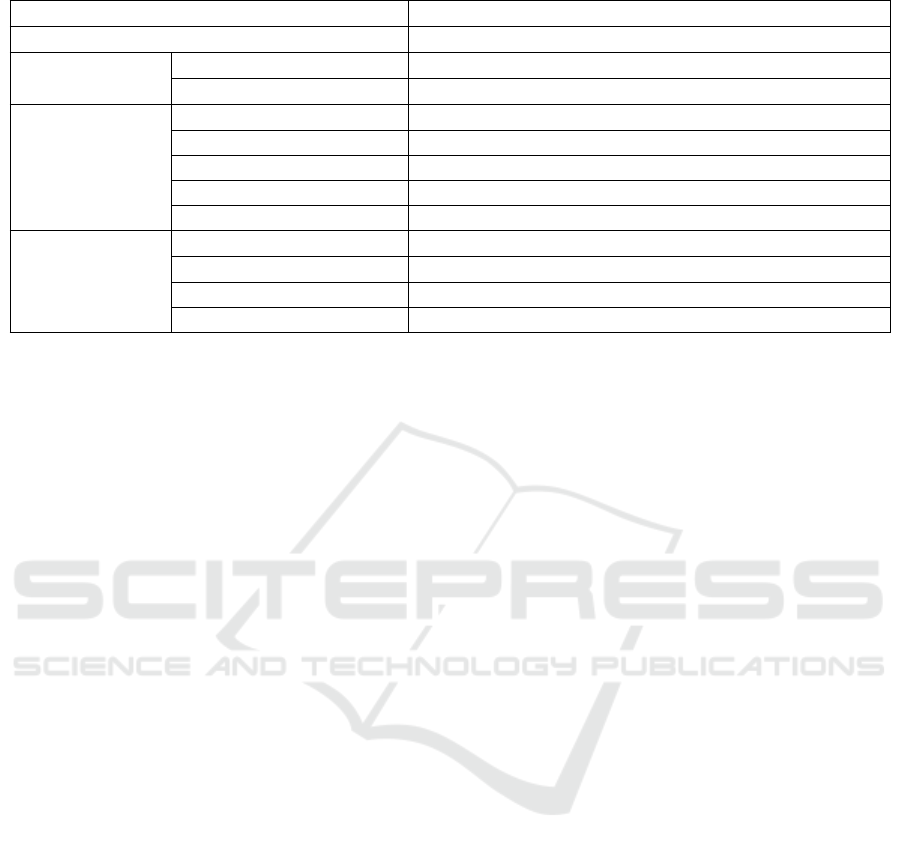
Table 1: Comparative Analysis of Related Works.
Related Work [1] [2] [3] [4] [5] [6] [7] [8] [9] [10]
Use of openEHR Archetypes • • • • • • • • • •
Health
Professionals
Participation ◦ ◦ ◦ • ◦ • • • • •
Considered End-Users • • • • • • • • • •
Modeling of
Archetypes with
Healthcare
Professionals
Requirements Analysis ◦ ◦ ◦ ◦ ◦ ◦ ◦ ◦ ◦ ◦
Prototyping ◦ ◦ ◦ ◦ ◦ ◦ ◦ ◦ ◦ ◦
Development ◦ ◦ ◦ ◦ ◦ • ◦ • • •
Validation ◦ ◦ ◦ ◦ ◦ ◦ • • • •
Not Specified • • • • • ◦ ◦ ◦ ◦ ◦
Focus Area
Clinical Standardization ◦ • ◦ ◦ • ◦ ◦ ◦ • ◦
Screening and Monitoring ◦ ◦ • ◦ ◦ • ◦ ◦ ◦ ◦
Decision Support ◦ ◦ ◦ • ◦ ◦ • • ◦ ◦
Clinical Use of EHR • ◦ ◦ ◦ ◦ ◦ ◦ ◦ ◦ •
Note: [1] = (Leslie, 2020); [2] = (Tian et al., 2021); [3] = (Li et al., 2020); [4] = (Silva et al., 2023); [5] = (Oliveira
et al., 2022); [6] = (Li et al., 2022); [7] = (Hak et al., 2020); [8] = (Li et al., 2021); [9] = (Wulff et al., 2021); and [10] =
(Arevshatyan et al., 2020).
of development can limit the adaptation of tools to
the reality of end users. This panorama, evidenced
by the analysis of the state of the art, indicates that
although openEHR archetypes offer a robust frame-
work for standardization, their effectiveness in repre-
senting the specialized knowledge of healthcare pro-
fessionals is compromised in the absence of a collab-
orative requirements elicitation process. Thus, the re-
search question highlights the need for more effec-
tive strategies for involving domain experts as early
as the elicitation phase, ensuring that the knowledge
of these professionals is reflected in the applications
developed.
5 USE OF ARCHETYPES BY
HEALTH PROFESSIONALS
This section explores the use of archetypes by health
professionals. It is divided into three stages. The
first stage outlines the evaluation scenario, detailing
the context and procedures followed during the ex-
periment. The second stage presents a quantitative
analysis of the statistical test results, focusing on the
responses. The final stage offers a qualitative study,
examining key points from the interviews and high-
lighting professionals’ perceptions, challenges, and
suggestions for improvement.
5.1 Evaluation Scenario
Our study involved 14 healthcare professionals di-
rectly engaged in patient care. We presented a sce-
nario focused on patient anamnesis and follow-up
processes. During anamnesis, essential patient in-
formation such as medical history, symptoms, and
lifestyle is gathered, while the follow-up phase moni-
tors progress and responses to treatment, aiding clini-
cal decisions.
The scenario was introduced to participants, and
we discussed the workflow to understand the de-
tails. Two archetypes representing anamnesis and
follow-up were presented, explaining data attributes,
terminologies, and constraints. Each professional
was encouraged to share opinions and ask questions,
leading to collaborative adjustments to ensure the
archetypes reflected the patient care scenario accu-
rately. Afterward, the graphical interface generated
from the archetypes was reviewed, and the impor-
tance of healthcare professionals’ involvement in re-
quirements elicitation was discussed. The profession-
als also completed a questionnaire, and the results are
presented in the next section.
5.2 Analysis of Quantitative Results
After applying the form, the data was analyzed using
the Wilcoxon test, which assesses whether a reference
value’s median differs significantly from zero. Imple-
mented in Python, the responses were compared to
the reference point 4, with results shown in the sec-
ond column of Table 2.
The first question, on method clarity, had a p-value
of 0.0005, indicating professionals found the method
straightforward. The second, on collaboration, had a
p-value of 0.0008, showing participants felt engaged
and able to contribute actively. The third, on the
archetype reflecting workflow understanding, had a
HEALTHINF 2025 - 18th International Conference on Health Informatics
676
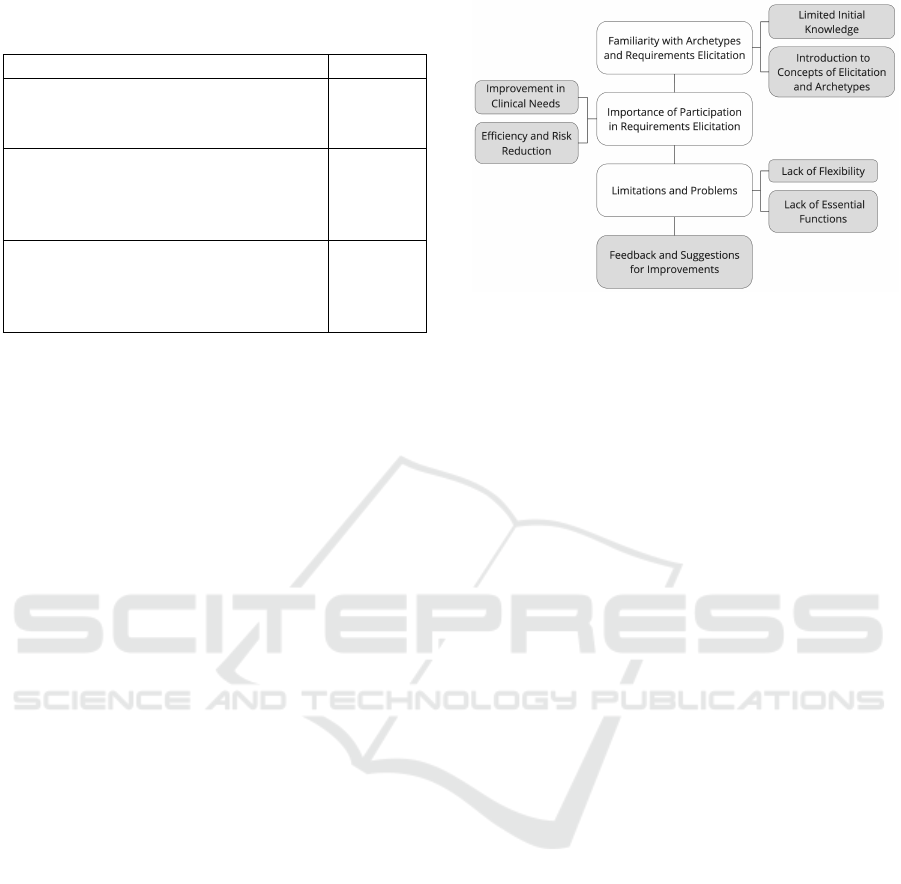
Table 2: Wilcoxon Test Results for Healthcare Profession-
als.
Question P-value
1. I believe that the method used to
identify the requirements was clear
and easy to follow.
0.0005
2. The method used to identify and
validate the requirements allowed me
to actively collaborate during the
requirements elicitation process.
0,0008
3. The data modeling represented by
the archetype facilitates my
understanding of the workflow in
which I am involved.
0,0013
p-value of 0.0013, demonstrating significant contri-
butions to understanding activity contexts.
These results highlight a positive perception of the
method, which is considered transparent, collabora-
tive, and effective, with high satisfaction among pro-
fessionals, meeting their expectations.
5.3 Analysis of Qualitative Results
During the experiment, various aspects were identi-
fied through content analysis to specify functionali-
ties in patient anamnesis and evolution systems using
archetypes. Participants’ perceptions and researchers’
observations provided insights into knowledge gaps
and challenges in enhancing understanding and en-
gagement. The analysis was organized into four key
moments. The first revealed participants’ limited ini-
tial knowledge of archetypes and requirements elic-
itation, leading to the introduction of fundamental
concepts. The second emphasized the importance
of healthcare professionals’ active participation in re-
quirements elicitation, highlighting benefits such as
improved clinical needs, efficiency, and risk reduc-
tion.
The third addressed limitations in existing sys-
tems and professionals’ need for tailored solutions,
demonstrating how well-designed systems improve
efficiency, precision, and satisfaction. Finally, the
fourth presented feedback and suggestions for im-
provement, as detailed in Figure 3.
• Familiarity with Archetypes and Require-
ments Elicitation
A key issue identified was the preconception that
healthcare professionals lacked familiarity with soft-
ware archetypes and requirements elicitation. This
was confirmed during interactions, highlighting the
need for clearer initial contextualization to explain
these concepts and better prepare participants.
Figure 3: Points of Perceptions and Contributions.
The tool was introduced, and doubts about pro-
fessionals’ involvement were clarified, emphasizing
their significant contributions. The fundamentals of
openEHR archetypes and the importance of active
participation to capture clinical needs were explained,
ensuring the elicitation process aligned with actual
demands. Professionals must understand their role
and development methodologies to avoid gaps in the
process.
Limited knowledge also created difficulties in
envisioning their role in requirements specification.
Without early intervention, this barrier can reduce
engagement, as technical terminology often makes
participants feel out of place. Addressing this re-
quires accessible language, explanations of funda-
mental concepts, and practical examples showing how
archetypes and the specification process benefit their
work.
• Importance of Participation in Requirements
Elicitation
After participating in the experiment, healthcare pro-
fessionals emphasized their value in the requirements
elicitation process, noting that their input is essential
for creating systems that meet clinical demands. One
participant stated, “Our presence is essential because
although you know very well how to develop the sys-
tem, you are not in practice to understand what our
real needs are,” underscoring that developers cannot
fully grasp clinical demands without firsthand experi-
ence.
The effectiveness of health applications depends
on both developers’ technical skills and direct feed-
back from end users. Professionals expressed concern
about ensuring the system supports specific tasks,
such as documenting essential information, customiz-
ing fields for specialties, and recording details like
allergies. During prototype analysis, one participant
suggested adding an ”allergies” field, emphasizing the
need for functionalities critical to clinical practice but
Integrating Clinical Expertise into Software Development: Evaluating the Use of openEHR Archetypes for Requirements Elicitation in
Healthcare Applications
677

easily overlooked in development.
Professionals also noted they often resort to paper
or manual processes due to the inflexibility of current
tools, which frequently fail to adapt to their needs.
• Limitations and Problems
Participants frequently reported challenges with cur-
rent software systems, which, despite being designed
for multi-professional use, rarely meet the specific
needs of all specialties. Healthcare professionals
highlighted limitations in electronic medical record
systems, which often fail to address their unique de-
mands. One participant remarked, “In the public ser-
vice, we get everything ready-made. [...] There are no
tools to open the system and find specific resources
for each profession.”
The inability to support multiple specialties was a
recurring frustration. In hospitals and public health
centers, a system equally effective for psychologists,
nutritionists, and other professionals is crucial. How-
ever, current systems often lack this flexibility, forc-
ing informal adaptations and note summarizations
that compromise care quality and patient records.
Ethical and data security issues were also noted, par-
ticularly regarding privacy and the risk of inappropri-
ate sharing between specialties. Participants stressed
the need for systems with controls to limit access to
sensitive information based on professional bound-
aries.
Professionals highlighted that their inclusion in
system development could address these issues, en-
suring each specialty’s needs are integrated from the
start. By participating in the requirements elicitation
process, they can identify essential functionalities for
their practices, creating flexible and practical systems.
Additionally, they pointed out that mere training in
tool usage is insufficient, as the challenges stem from
structural and functional limitations beyond usability.
• Feedback and Suggestions for Improvements
After completing the survey, participants shared im-
pressions of the specification process and tool, ex-
pressing positive experiences while suggesting im-
provements. A key observation was the need for more
time, ideally available in real environments, as the ex-
periment’s simulated context limited time.
A prominent suggestion was improving the
graphic interface for a more intuitive and visually or-
ganized design. Simpler navigation for locating and
filling in fields could enhance efficiency and reduce
cognitive load, making the specification process more
agile. One participant remarked, “With a prettier in-
terface, it would be much easier to use and even more
intuitive.”
This is particularly relevant given the technical
complexity of openEHR archetypes. While designed
to represent clinical data accurately, the current in-
terface can be challenging for users unfamiliar with
specific health concepts. A more intuitive design
could make openEHR more accessible, enabling pro-
fessionals to focus on specifying functionalities with-
out unnecessary distractions or difficulties.
6 FINAL CONSIDERATIONS
This article demonstrates that using openEHR
archetypes in requirements elicitation and specifica-
tion effectively integrates healthcare professionals’
specialized knowledge into clinical systems develop-
ment. The literature review revealed a significant
gap in involving these professionals during require-
ments elicitation, particularly in studies incorporating
archetypes.
The results indicate a positive perception among
health professionals, highlighting clarity, collabora-
tion, and effectiveness. Participants considered the
process transparent and engaging, with opportunities
to define and validate requirements. Modeling with
archetypes facilitated understanding activities, con-
firming a collaborative approach aligned with profes-
sional expectations. These findings show the method-
ology effectively integrates healthcare professionals’
knowledge. However, limitations included healthcare
professionals’ unfamiliarity with the technology, em-
phasizing the need for robust educational support on
openEHR archetypes and their role. Limited time for
demonstrating and specifying functionalities in the
simulated environment may have impacted contribu-
tions.
Future recommendations include expanding ex-
periments to a diverse healthcare professional sam-
ple across specialties and experience levels, en-
abling comprehensive analyses of challenges and
needs. Including varied profiles—doctors, nurses,
managers, and technicians—could reveal differences
in archetype use, aiding in versatile system develop-
ment. Formalizing good practices for archetype use
through guides, checklists, and manuals is also essen-
tial, alongside applying these practices in real devel-
opment environments to assess effectiveness, observe
user-developer interactions, and adjust as needed.
This study’s limitations include a small sample
size, controlled environment, professionals’ unfamil-
iarity with archetypes, and limited time for specifica-
tion, which restrict generalization to all clinical con-
texts or profiles.
HEALTHINF 2025 - 18th International Conference on Health Informatics
678

REFERENCES
Arevshatyan, S., Burriel, V., Bosc
´
a, D., Reyes, J. F., Pastor,
´
O., Yoffe, I., Denis, R. M. C., Gauna, C. V., Sforza,
S., Ayala, S. J., et al. (2020). An application of an ehr
based on conceptual modeling to integrate clinical and
genomic data and guide therapeutic strategy. In Anales
de la Facultad de Ciencias M
´
edicas, volume 53, pages
17–30.
Badr, N. G. (2019). Guidelines for health it addressing the
quality of data in ehr information systems. In Health-
inf, pages 169–181.
Barbosa, S. D. J., Silva, B. d., Silveira, M. S., Gasparini,
I., Darin, T., and Barbosa, G. D. J. (2021). Interac¸
˜
ao
humano-computador e experi
ˆ
encia do usuario. Auto
publicac¸
˜
ao.
Bitkina, O. V., Kim, H. K., and Park, J. (2020). Usability
and user experience of medical devices: An overview
of the current state, analysis methodologies, and fu-
ture challenges. International Journal of Industrial
Ergonomics, 76:102932.
Chen, R., Klein, G. O., Sundvall, E., Karlsson, D., and
˚
Ahlfeldt, H. (2009). Archetype-based conversion of
ehr content models: pilot experience with a regional
ehr system. BMC medical informatics and decision
making, 9:1–13.
da Silva, M. A. P., Times, V. C., de Ara
´
ujo, A. M. C.,
and da Silva, P. C. (2019). A microservice-based ap-
proach for increasing software reusability in health
applications. In 2019 IEEE/ACS 16th International
Conference on Computer Systems and Applications
(AICCSA), pages 1–8. IEEE.
de Ara
´
ujo, A. M. C., Times, V. C., da Silva, M. U., Alves,
D. S., and de Santana, S. H. C. (2016). Template4ehr:
building dynamically guis for the electronic health
records using archetypes. In 2016 IEEE International
Conference on Computer and Information Technology
(CIT), pages 26–33. IEEE.
de Ara
´
ujo, A. M. C., Times, V. C., and Silva, M. U.
(2019). Towards a reusable framework for generat-
ing health information systems. In 16th International
Conference on Information Technology-New Genera-
tions (ITNG 2019), pages 423–428. Springer.
Ding, Y., Hu, Z., Wang, Y., Xu, X., Nan, S., and Duan,
H. (2023). Accelerate clinical decision support sys-
tem development by converting ontology to openehr
archetypes. In 2023 9th International Conference on
Big Data and Information Analytics (BigDIA), pages
372–378. IEEE.
Ferreira, D. E. and de Souza, J. M. (2023). Methodology for
developing openehr archetypes: a narrative literature
review. Journal of Health Informatics, 15(2):53–59.
Foundation, O. (2023). Clinical knowledge manager (ckm)
archetype repository. Accessed: 2024-10-12.
Govella, A. (2019). Collaborative Product Design: Help
Any Team Build a Better Experience. O’Reilly Media.
Hak, F., Oliveira, D., Abreu, N., Leuschner, P., Abelha, A.,
and Santos, M. (2020). An openehr adoption in a por-
tuguese healthcare facility. Procedia Computer Sci-
ence, 170:1047–1052.
Leslie, H. (2020). openehr archetype use and reuse within
multilingual clinical data sets: case study. Journal of
medical Internet research, 22(11):e23361.
Li, M., Cai, H., Nan, S., Li, J., Lu, X., and Duan, H. (2021).
A patient-screening tool for clinical research based on
electronic health records using openehr: development
study. JMIR Medical Informatics, 9(10):e33192.
Li, M., Cai, H., Zhi, Y., Fu, Z., Duan, H., and Lu, X.
(2022). A configurable method for clinical quality
measurement through electronic health records based
on openehr and cql. BMC Medical Informatics and
Decision Making, 22(1):37.
Li, M., Leslie, H., Qi, B., Nan, S., Feng, H., Cai, H., Lu,
X., and Duan, H. (2020). Development of an openehr
template for covid-19 based on clinical guidelines.
Journal of medical Internet research, 22(6):e20239.
Maramba, I., Chatterjee, A., and Newman, C. (2019). Meth-
ods of usability testing in the development of ehealth
applications: a scoping review. International journal
of medical informatics, 126:95–104.
Moner, D., Maldonado, J. A., and Robles, M. (2018).
Archetype modeling methodology. Journal of
biomedical informatics, 79:71–81.
Oliveira, D., Santos, A., Braga, D., Silva, I., Sousa, R.,
Abelha, A., and Machado, J. (2022). Openehr mod-
elling applied to complementary diagnostics requests.
Procedia Computer Science, 210:265–270.
openEHR Foundation (2024a). openEHR Specifications:
Archetype Model, Release 2.3.0. Accessed: 2024-11-
04.
openEHR Foundation (2024b). openEHR Specifications:
Reference Model, Release 1.1.0. Accessed: 2024-11-
04.
Palojoki, S., Lehtonen, L., Vuokko, R., et al. (2024). Se-
mantic interoperability of electronic health records:
Systematic review of alternative approaches for en-
hancing patient information availability. JMIR med-
ical informatics, 12(1):e53535.
Silva, I., Ferreira, D., Peixoto, H., and Machado, J. (2023).
A data acquisition and consolidation system based on
openehr applied to physical medicine and rehabilita-
tion. Procedia Computer Science, 220:844–849.
Silva, J., Ara
´
ujo, A., Coutinho, F., and Silva, A. (2024). Are
end-users participating in the life cycle of healthcare
application development? an analysis of the opportu-
nities and challenges of the use of hci techniques in
the healthcare sector. BIOSTEC (2), pages 789–796.
Tian, Q., Han, Z., Yu, P., An, J., Lu, X., and Duan, H.
(2021). Application of openehr archetypes to auto-
mate data quality rules for electronic health records:
a case study. BMC Medical Informatics and Decision
Making, 21:1–11.
Wulff, A., Baier, C., Ballout, S., Tute, E., Sommer, K. K.,
Kaase, M., Sargeant, A., Drenkhahn, C., Schl
¨
uter, D.,
et al. (2021). Transformation of microbiology data
into a standardised data representation using openehr.
Scientific Reports, 11(1):10556.
Integrating Clinical Expertise into Software Development: Evaluating the Use of openEHR Archetypes for Requirements Elicitation in
Healthcare Applications
679
