
A Group Activity Based Method for Early Recognition of Surgical
Processes Using the Camera Observing Surgeries in an Operating
Room and Spatio-Temporal Graph Based Deep Learning Model
Keishi Nishikawa
1
and Jun Ohya
2
1
Global Information and Telecommunication Institute, Waseda University, 3-4-1, Okubo, Shinjuku, Japan
2
Department of Modern Mechanical Engineering, Waseda University, 3-4-1, Okubo, Shinjuku, Japan
Keywords: Graph Processing, Early Recognition, Surgical Process, Operating Room.
Abstract: Towards the realization of the scrub-nurse robot, this paper proposes a group activity-based method for the
early recognition of surgical processes using an early part of the video acquired by the camera observing
surgeries. Our proposed method consists of two steps. In the first step, we construct a spatial-temporal graphs
which represents the group activity in operating room. The graph’s node contains (a) the visual features of
participants and (b) the positions. In the second step, the generated graphs are input to our model for
classification of the input. In our model, since the generated graph’ node contains both visual features and the
position information, we treat the graph as the point cloud in spatial-temporal space. Therefore, Point
Transformer Layer from (Zhao et al., 2021) is used as the building block. Experiments are conducted on
public datasets; (Özsoy et al., 2022)’s mock surgery of knee replacement. The results show our method
performs early recognition achieving the accuracy of 68.2 %~90.0 % in early duration such as 17.1 % ~
34.1 % of the entire durations from the beginning on the dataset. Furthermore, the comparison with the state-
of-the-art method (Zhai et al., 2023) in early recognition of group activity is also conducted. It turns out that
ours outperforms (Zhai et al., 2023) significantly.
1 INTRODUCTION
In general, a surgery is conducted with the
cooperation of both many surgeons and nurses.
Towards keeping the surgery forward smoothly, the
nursers often observe the situation, recognize the
necessary instruments and information, and pass them
to the surgeons. However, according to the
investigation by The Japan Institute for Labour Policy
and Training, the shortage of the nurses is a serious
problem (The Japan Institute for Labour Policy and
Training, 2022). To relax this problem, it is necessary
to achieve systems that work as alternatives of the
nurses. (Li et al., 2016) indicate that the requirements
of such a system include to recognize and make the
appropriate decisions for supporting the surgeons
autonomously, without any external operation by the
surgeons, being able to recognize the surgical process
and the actions as early as possible to pass the
necessary instruments to the surgeons, and so on.
As shown in Fig. 1, the surgery consists of
multiple surgical processes, and each of the surgical
processes consists of one or more surgical actions,
forming a kind of hierarchical relationship among the
surgical processes and actions. The level shown in
Fig.1 means the granularity in the hierarchy. Note that
the process is at the higher level than the action. In (Li
et al., 2016), the surgical actions to be recognized
have been focused on the hand actions which relates
to the requirement of passing the instrument to the
surgeons towards replacing the nurses. However, it is
also necessary to do the following things in addition
to passing surgical tools.
1) Providing useful information about the
cautions and the roles of the participants to the
surgery.
2) Recognizing the emergencies that occurred
during the surgical process and controlling the robots
to help the surgeons avoid the difficult situation.
For achieving the above points, it is necessary to
recognize the surgical process. In the view of
providing the support for the surgery, each surgical
process and action must be recognized as early as
possible. Even though each surgical process consists
712
Nishikawa, K. and Ohya, J.
A Group Activity Based Method for Early Recognition of Surgical Processes Using the Camera Observing Surgeries in an Operating Room and Spatio-Temporal Graph Based Deep Learning
Model.
DOI: 10.5220/0013252700003905
In Proceedings of the 14th International Conference on Pattern Recognition Applications and Methods (ICPRAM 2025), pages 712-724
ISBN: 978-989-758-730-6; ISSN: 2184-4313
Copyright © 2025 by Paper published under CC license (CC BY-NC-ND 4.0)
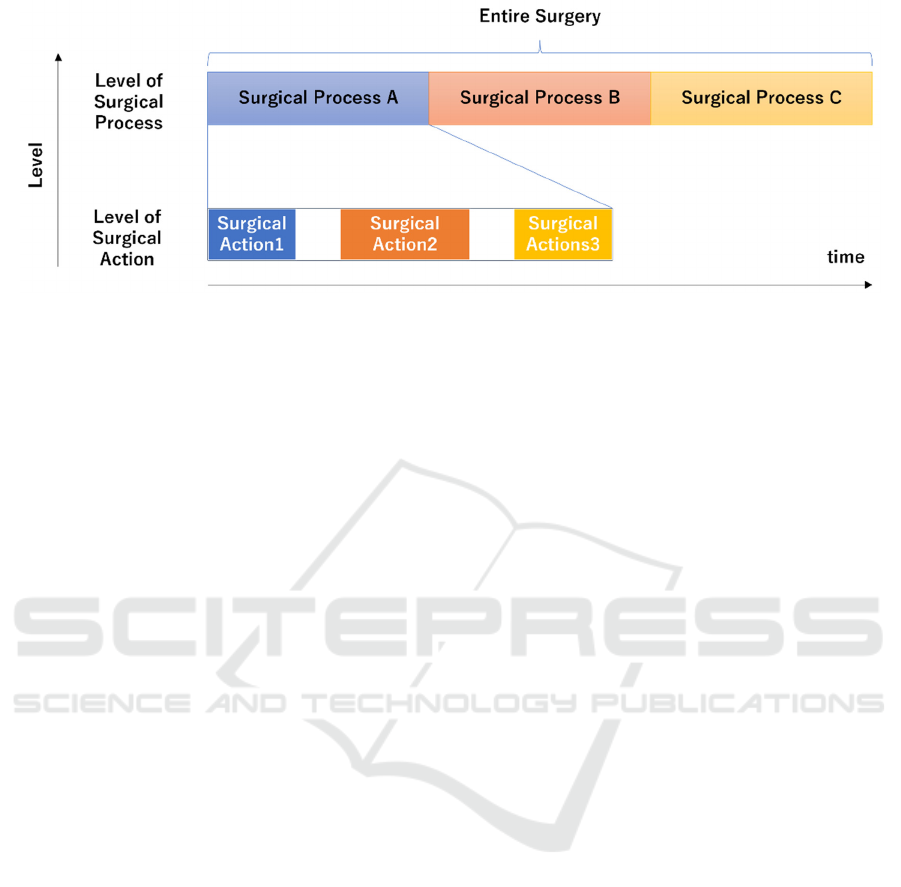
Figure 1: Flow of the surgery and the levels of the elements consisting of the surgery.
of multiple surgical actions, it is highly possible
that multiple surgical processes could contain same
surgical actions. Therefore, recognizing surgical
actions is not sufficient for recognizing surgical
processes.
One of the important features of the surgery is that
the surgeons and the nurses could cooperate and
interact with each other. Therefore, although the work
(Li et. al, 2016) recognizes individual’s actions, that
is not sufficient for recognizing the surgical process,
as mentioned earlier. To solve this issue, the motions ,
the positions, and the number of the participants in the
operating room can be useful. Therefore, it is
reasonable that the positions and motions of the
participants as groups at each time instance are
captured and used for the early recognition of surgical
processes. For collecting that kind of information, a
bird-view camera which can capture the entire space
of the operating room is appropriate.
While some works about surgical process
recognition have been conducted in the form of
surgical phase classification or surgical activity
recognition using videos acquired by the camera
installed in an operating room (K. Yokoyama et al.
2023), (E. Özsoy et al. 2024), (E. Özsoy et al. 2023),
(Shargi et al., 2020), (L. Bastian et al., 2022), these
did not focus on early recognition. Therefore, to best
our knowledge, early recognition of activities in an
operating room has not been researched well.
Furthermore, dataset collected in the community of
surgical data science tends to be small compared to
that in the community of computer vision due to
privacy issue etc.
In this paper, a method for early recognition of the
surgical process using a bird-view camera in the
operating room is proposed. The proposed method
consists of the following two modules: (1)
constructing the spatial-temporal graphs which
represents not only visual features of the participants
but also the positions and the number of participants
of the surgery and (2) processing the graph generated
during early duration of the input video to classify it
as one of the surgical processes by our model which
consists of graph neural networks layer. Especially
the model utilizes Point Transformer Layer as the
building blocks to deal with the graphs which has the
geometric information in spatial-temporal space. For
conducting experiments, we used publicly released
video dataset which observes mock surgery of knee-
replacement.
2 RELATE WORK
2.1 Conventional Works
In case of action recognition, the goal is to recognize
the action using the video data captured from the
beginning to the end. However, in case of early
recognition, the input to the recognition model is an
early part of the video data: from the beginning to an
early time instance before the end. According to the
survey (H Zhao et al., 2021), the conventional works
can be classified into the three main categories: (1)
One-Shot based method, (2) Knowledge Distillation
based method, and (3) Propagation based method.
2.1.1 One-Shot Based Method
The methods in this category do not take the fully
observed information as the input, but the partially
observed information which means the early part of
the video as the input (Zhou et al, 2018), (Chen et al.,
2018), (Singh et al., 2017), (Sun et al., 2019). (Zhou
et al, 2018) exploit the features extracted from the
entire area of the image. (Chen et al., 2018) focus on
the joints of a person in the given video and weight
the features of the local region which surrounds the
A Group Activity Based Method for Early Recognition of Surgical Processes Using the Camera Observing Surgeries in an Operating Room
and Spatio-Temporal Graph Based Deep Learning Model
713

joints for improving the recognition of the action in
the early stage. The method proposed by (Singh et al.,
2017) detects the rectangle which surrounds the
person in the video and achieve the early action
recognition in real time setting by accumulating the
detections over the temporal domain. (Sun et al.,
2019) also detect the multiple people in the image and
create the graphs whose node contains the feature,
which is extracted from the detections: the graph is
used for representing the relationship among the
multiple people in the image.
2.1.2 Knowledge Distillation Based Method
Although only the partial observed information is
used for the inference, both the full and partial
information are used for the training. In this setting,
the methods proposed in (Ma et al., 2016),
(Aliakbarian et al., 2017) construct the model for
increasing the confidence of the recognition as the
observed information increases by the temporal
progress. In (Aliakbarian et al., 2017) (Kong et al,
2017), the mapping function is learned by
approximating the fully observed information with
the partial information for improving the recognition
at the early stage of the action.
2.1.3 Propagation Based Method
The methods in this category use the generative
model for generating the data which will be likely to
be observed in the future based on the partially
observed information. One of the representative
works in this category is the work by (Zhao et al.,
2019).
2.1.4 Early Recognition of Group Activity
While many of the methods in the above categories
are targeting at actions done by one person or
targeting at scenes in which the actions are not treated
as group actions, there is a work for recognizing
group actions at the early stage.
(Chen et al., 2020) exploits two graphs for the
input. The first graph represents the positions of the
people and the relationship among the people. The
second graph represents the features of the action of
each person and the relationship based on the
similarities among the actions. They use two types of
autoencoders for extracting the features from both
graphs respectively. The encoders are learned with
the adversarial loss to approximate the fully observed
information with the partially observed information.
Chen et al. validate the effectiveness of their method
for the early recognition of group actions in the
volleyball and daily actions such as walking. They
also note the predicting the positions is important to
capture the group action.
(Zhai et al., 2023) also propose a method for early
recognition of group actions. In (Zhai et al., 2023), a
virtual leader node which connects to each individual
node in the group is added to the graph while Chen et
al. (Chen et al., 2020) focus on the pair-wise
connection among the group. By setting virtual leader
node, (Zhai et al., 2023) can summarize the group-
wise representation. Also, (Zhai et al., 2023) do not
require fully observed information for learning as
opposed to (Chen et al., 2020).
Based on the above survey and our purpose, it is
natural to consider that our method belongs to the
works which are introduced in this section, that is
early recognition of group activity. While there are
many works about the recognition of group activity
which recognize the activity based on the fully
observed information (Wu et al, 2019), (Li et al.,
2021), not many works on early recognition of group
activity can be seen: to best our knowledge, (Chen et
al., 2020) and (Zhai et al., 2023) are the only works.
However, (Chen et al., 2020) and (Zhai et al., 2023)
are targeting at general group activities, as opposed to
our target at group activities in operating rooms.
2.1.5 Activity Recognition in Operating
Room and Dataset
Conventional works about action/activity recognition
(not early recognition) in an operating room have
been conducted (Yokoyama et al., 2023), (Özsoy et
al., 2024), (Shargi et al., 2020), (Bastian et al., 2022).
(Yokoyama et al., 2023) proposed a method for the
detection of passing a medical instrument and group
attention during surgery by utilizing pose estimation
of the participants. Experiments are conducted by
using six videos capturing real surgeries by a camera
attached to the ceiling of the operating room.
(Shargi et al., 2020) proposed a method for
surgical activity recognition in an operating room in
which they assume robot-assisted surgery would be
conducted. They took video clips as the input from
which features are extracted by a deep learning model
and correlated the features to temporal contexts. They
collected 400 videos captured by multiple time of
flight cameras attached to the operating room. The
size of their dataset could be the largest in the
community of surgical data science, but the dataset is
not released publicly.
(Özsoy et al., 2022) and (Özsoy et al., 2024)
released the dataset which captures the simulated
surgery of total knee replacement by multi-view
ICPRAM 2025 - 14th International Conference on Pattern Recognition Applications and Methods
714

RGB-D cameras in an operating room. The dataset is
called 4D-OR, which is the first publicly released
dataset capturing the surgery in OR (an operating
room) according to (Özsoy et al., 2022). In (Özsoy et
al., 2022) they proposed a method for generating
semantic scene graphs in the operating room and
utilizing the graphs for predicting the roles of the
participants in the surgery. They captured 10
surgeries for the dataset. Moreover, in (Özsoy et al.,
2024) they extended their work (Özsoy et al., 2022)
by adding the surgical phase recognition to the
downstream tasks.
(Bastian et al., 2022) investigated the modalities
of the input to the deep learning model for surgical
action classification and which method for fusing
them makes the best performance. In (Bastian et al.,
2022), the modalities are RGB, depth and infrared
because they use Asure Kinect Camera (Microsoft,
2021) which can capture RGB, Depth and Infrared
images. They collected 16 videos of laparoscopic
interventions in multi-view setting. They found that
combination of RGB and Depth and late fusion of
RGB and Depth made the best performance for
surgical action classification.
To summarize, although the action/activity
recognition in an operating room to which the camera
is attached and capturing the surgeries in bird-view or
objective-view are researched frequently, early
recognition of group activity in an operating room is
not conducted in the community of surgical data
science. In addition to that, it is obvious that the
dataset collected in the operating room towards the
research in the community is much smaller than that
in the community of the computer vision except
(Shargi et al., 2020). Although the dataset collected in
(Shargi et al., 2020) is much larger than those in the
others, it is not publicly available.
2.2 Problems in Conventional Works
In this paper, the goal is the early recognition of the
surgical process. Based on our observation, the two
characteristic points of the surgical process are found.
(A) The surgical process is a lengthy operation
lasting from tens of minutes to several hours.
(B) The surgical process is carried out
simultaneously by multiple participants,
including the surgeons, assistants, and
nurses. Since each participant works at
his/her own position in the operating room to
play his/her own role. The number of the
participants dynamically changes depending
on the surgical process. Not only the visual
features of the participants but also the
position and the number for those can be
distinguishable ques of activity in early
stage.
In terms of the above-mentioned (A) and (B), the
conventional works have the following problems.
In general, they used the datasets (Soomro et al.,
2012), (Jhuang et. al, 2013), (Kong et al, 2012),
(Patron-Perez et. al, 2010), (Goyal et. al, 2017), (Hu
et al., 2017), (Y. Li , C. Lan and et. al, 2016), (Liu et
al., 2017), which comprise short actions.
Furthermore, both the knowledge distillation-based
method and the propagation-based method use not
only the partial information but also the fully
observed information. In addition, the surgery takes a
few hours: i.e. the duration of the surgery is much
longer than that of the actions in the above-mentioned
datasets. Therefore, the amount of the features
increases as the observed frames increases. Though
LSTM (Long Short Term Memory), which is often
used, processes the temporal dynamics of the features
(Ma et al., 2016), (Aliakbarian et al., 2017), it is
difficult to build a realistic model that deals with
temporally much longer data in a reasonable fashion.
The reason is the low efficacy of the learning as
pointed out in (Bradbury et al., 2016), while the
learning in parallel is difficult.
The methods without using LSTM (Kong et al,
2017) and (Kong et al., 2014) divide the full-observed
information into multiple partial information in the
temporal dimension. After the division, multiple early
image data are stacked to the matrix. In the learning,
the mapping function is learned by approximating the
stacked early image data matrix to the full-
information matrix. This processing is affected by the
temporal width (duration) of each division. In case of
the smaller width, the temporal dimension of the
stacked information gets larger because the amount of
the features from the set of the partial information
increases. That causes the computation during the
learning to be difficult. In case of the larger width, the
division gets coarser. This leads to the deterioration
of the capability of the features to represent the action
because the one feature corresponds to the early but
long duration, which means that the information of
the long duration is compressed into the one vector
which constructs the early image data matrix.
One shot based methods use the short-duration
information to recognize the actions. The input is the
features extracted from the entire region (Zhou et al,
2018) or from the local region which surrounds the
joints of the person (Chen et al., 2018), while those
methods do not utilize the positions of people
explicitly for building their models. In the videos
capturing multiple persons’ actions, (Singh et al.,
A Group Activity Based Method for Early Recognition of Surgical Processes Using the Camera Observing Surgeries in an Operating Room
and Spatio-Temporal Graph Based Deep Learning Model
715

2017) detected the area of each person and
represented the graph by connecting the detections.
However, the node of the graph is the feature
extracted from the areas of the detections and they
focus on the relationship. Therefore, Singh et al.
(Singh et al., 2017) do not utilize the positions and the
motions of the people in the video either.
Although the camera in the operating room
captures the entire area of the room, these methods
cannot deal with the recognition capturing the
characteristics described as the above-mentioned
feature (B). The reason is that they extract the features
from the entire region of the image, however, they do
not embed the contribution of each person for group
activity in the image explicitly.
In (Chen et al., 2020), which is a major work and
similar one to ours in terms of early recognition of
group activities, (Chen et al., 2020) represented the
actions of the group using a graph-structure. They
used multiple auto-encoders that are learned based on
the partial information that is represented by a spatio-
temporal graph. As mentioned above, longer videos
tend to cause the problem which is similar to the one
of (Kong et al, 2017) and (Kong et al., 2014). In
addition to that, (Chen et al., 2020) uses both full and
partial information for computing the adversarial loss.
This also makes the computation difficult. In (Chen
et al., 2020), their targets are short-duration-actions
of groups such as spikes in volleyball (Ibrahim et al,
2016) and daily activities (Choi et al., 2009),
including walking. The durations of these actions are
about a few seconds, but, on the other hand, the
dataset (Özsoy et al., 2022) which simulates the
surgery contains processes whose durations are more
than 1 minutes.
(Zhai et al., 2023) do not need the fully observed
information for building the model and achieve state
of the art performance on the datasets introduced by
(Ibrahim et al, 2016) and (Choi et al., 2009). (Zhai et
al., 2023) introduced a virtual leader node into a graph
which represents the group activity. The node
represents the summarization of the features of
member’s action by gathering visual feature vector
from member’s area in each frame. Furthermore,
(Zhai et al., 2023) introduced Group Residual module
which exploits the idea of virtual leader node for
processing the graph. As a result, (Zhai et al., 2023)
outperform (Chen et al., 2020) using the dataset of
(Ibrahim et al, 2016) and (Choi et al., 2009) because
(Zhai et al., 2023)’s method successfully captures
characteristic points of group activity.
(a)
(b)
Figure 2: Examples of the images from surgical processes
in (Özsoy et al., 2022).
However, (Zhai et al., 2023) did not consider the
position and the number of the participants in each
frame and balance among them. In this paper, note
that members correspond to participants of surgeries.
In the operating room, the participants have their own
roles needed for accomplishing the surgical process,
and the positions, the number and those variation are
different from each other. This problem belongs to
(B) because members’ contribution and the temporal
variation relates to the role of the members. In this
paper, the method is proposed for early recognition to
solve the problems (A) and (B): that is, the proposed
method utilizes the motions, the potions and the
number of the participants in the operating room.
3 PROPOSED METHOD
3.1 Our Basic Idea
As a result of our observations to the mock surgery
(Özsoy et al., 2022), the following two points are
found; (1) early recognition of surgical process in
operating room is that of group activity in operating
room, and (2) cues for early recognition are not only
the visual features of the participants but also the
ICPRAM 2025 - 14th International Conference on Pattern Recognition Applications and Methods
716
positions and the number of the participants. It is
natural to assume that the visual features represent
how the participants do their own task during the
surgical process. In addition to that, the positions and
number vary among the surgical processes. The
examples are shown in Fig. 2. In Fig 2 (a), two
participants are doing the task close to the table and
the other participant is watching the scene at a place
away from the two. On the other hand, in Fig 2 (b)
there are four participants, and their positions are
different from those in (a).
To reflect the visual features, the positions and the
number of the participants for early recognition, the
graph whose node represents the visual feature and
the position of a participant is built at each frame and
it is accumulated along the temporal progress so that
the spatial-temporal graph is acquired. The number of
participants is represented by the number of nodes in
the graph at each frame. Here, from the point of view
in geometric shape, the spatial-temporal graph can be
regarded as point cloud data with other modal
information such as visual feature at each point
because the node has the position information
therefore it can be viewed as point in space.
Furthermore, the variation of the number, the position
of the node and the temporal variation in the spatial-
temporal graph can be the shape of point cloud data
in spatial-temporal space. Based on the idea, a model
which is used by our method is built based on graph
neural networks which can process the input graph
considering the property of the point cloud.
While our method is similar to (Chen et al., 2020)
in terms of using spatial-temporal graph including the
visual features and the 2D positions of the
participants, our method is different from (Chen et al.,
2020) because the graph contains the visual features,
the positions of the participants in each frame and the
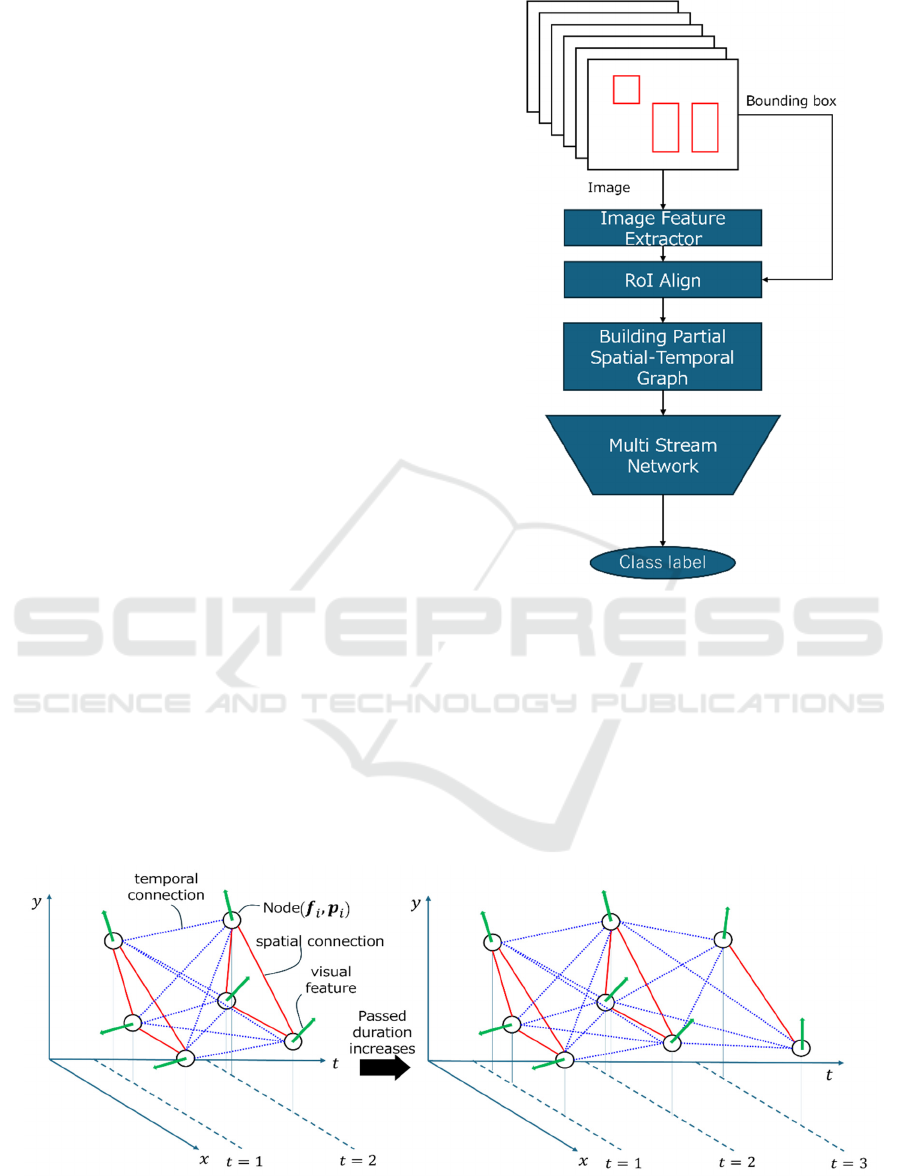
Figure 3: The entire flow of our proposed method.
time instance which corresponds to each frame in the
form of the point cloud. In addition to that, ours
differs from (Chen et al., 2020) in processing the
graph because (Chen et al., 2020) treats the visual
features and position information separately and
process the two kinds of auto-encoders respectively,
while ours processes our spatial-temporal graphs by
utilizing the graph neural network which can deal
with our graph as point cloud.
Figure 4: Overview of Generation of Graph.
A Group Activity Based Method for Early Recognition of Surgical Processes Using the Camera Observing Surgeries in an Operating Room
and Spatio-Temporal Graph Based Deep Learning Model
717
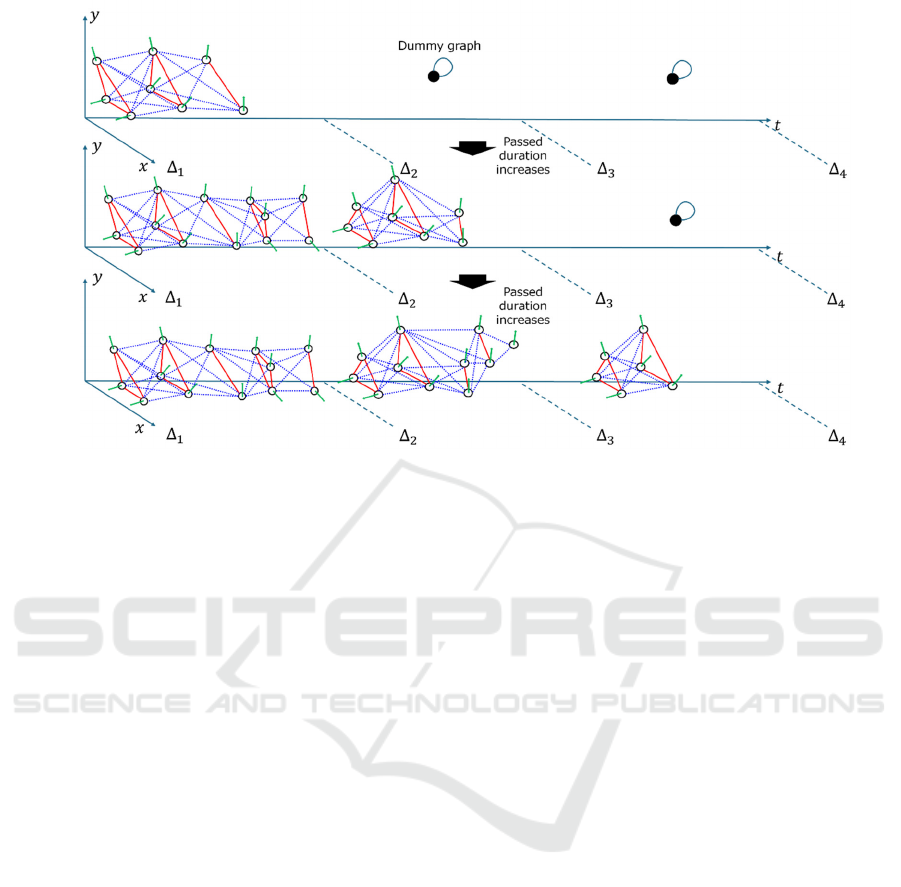
Figure 5: Generation of Patial Graph in which the number of temporal segments is three.
3.2 Flow of Our Proposed Method
The flow of our proposed method is shown in Fig.3.
The proposed method consists of two steps. In the
first step, the Spatial-temporal graphs are built. The
graph represents the activity of the group during the
partial duration. After building the graphs, these
graphs are fed into a model. The model infers the
class which the input graphs belong to. That is, we
formulated the problem of early recognition of group
activity in operating room as the classification of the
spatial-temporal graph which is generated from video
frames observed in early part.
3.3 Graph Construction
In this section, the process for making these graphs is
explained. Note that it is assumed that the detections
of the participants in each frame are obtained in
advance.
3.3.1 Basic Idea of Generating Graph
The procedure for making the graph from the
observed video frames is shown in Fig 4.
In the first step, the visual feature is extracted
from the local area corresponding to the bounding
box which surrounds each participant in the feature
map of each frame by using RoI-Align(He et al.,
2017). At the same time, the centre coordinates of the
bounding boxes are also recorded as the geometric
information.
In the second step, the visual feature and
geometric information of each person are associated
with a node of the graph. Note that, in this step, the
time instance is added to the geometric information
so that the geometric information has the 3D
information which consists of the 2D point in the
image and time instance in the spatial-temporal space.
The node contains the visual features and position
information so that the node can be treated as a 3D
point with other modal information such as RGB
information in point cloud data acquired by RGB-D
camera.
In the graph, the nodes are connected to each other
in a bi-directional manner. In summary, the above-
mentioned graph is represented by Eq. (1).
𝐺
=(𝑉
,ℇ
)
𝑉
=
(
𝒇
,𝒑
)
|
|
𝒇
=𝑅𝑜𝐼𝐴𝑙𝑖𝑔𝑛(𝑭
),𝒑
=
(
𝑥
,𝑦
,𝑡
)
∈𝑅
ℇ
=𝑒
,
(1
)
where 𝐺
is a graph whose nodes and edges are 𝑉
and ℇ
, respectively. 𝑉
has the visual features 𝒇
and
position vector 𝒑
, where 𝑖(= 1,…,
|
𝑉
|
) is the index
of a node. The visual feature is the output of
𝑅𝑜𝐼𝐴𝑙𝑖𝑔𝑛 of feature map 𝑭
. The position vector 𝒑
is
the three-dimensional vector whose elements are the
coordinates (𝑥
,𝑦
) of the centroid of the bounding
box, and the time instance 𝑡 in which the
corresponding frame is observed. 𝑒
,
is the edge
between 𝑗-th node and 𝑘-th node. As the time
ICPRAM 2025 - 14th International Conference on Pattern Recognition Applications and Methods
718
instance 𝑡 passes, the spatial-temporal graph grows as
shown in Fig 4. Thus, the variation of the number and
position of the point is represented by changes in the
geometric shape of the graph spatial-temporal space.
3.3.2 Partial Spatial-Temporal Graph
Although the graph which can represent the shape in
the spatial-temporal dimension is constructed, there is
possibility that the geometric shape of the graph is not
considered sufficiently because our model whose
building block is Point Transformer Layers processes
the entire structure of the graph and ignore the local
feature. To deal with this issue, we divide the spatial-
temporal graph into a few sub-graphs. Concretely, the
sub-graphs are built in each equally-divided duration.
In the following, the equally-divided duration is
called “temporal segment”. For example, in case of
that the entire duration is 30 seconds with three
temporal segments, the first, second and third
temporal segments correspond to from 1 to 10
seconds, from 11 to 20 seconds and from 21 to 30
seconds respectively. The sub-graph is generated
based on the frames in each temporal segment. If 𝑡
10 seconds, in the temporal segment corresponding
to duration from 1 to 10, the spatial-temporal graphs
is acquired by accumulating spatial-graphs over the
temporal dimension: i.e. for accumulating the graphs
over temporal dimension, the nodes obtained from the
new observed frame are appended to the already built
graphs, and the new nodes are connected to the nodes
in the already built graph. Note that the spatial and
temporal connections among the nodes is full and bi-
directional.
In other temporal segments in which the current
time instance is before the start of the temporal
segment, the dummy graph, which contains only one
node having a zero vector with self-connecting edge,
is generated.
In summary, the above-mentioned processes are
represented by Eq. (2).
𝐺
,
,
=
𝑉
,ℇ
if Δ
𝑡 Δ
(
𝑉
,ℇ
)
else 𝑡Δ
𝑉
=
(
𝒇
,𝒑
)
𝒇
=𝑅𝑜𝐼𝐴𝑙𝑖𝑔𝑛(𝑭
),𝒑
=
(
𝑥
,𝑦
,𝑡
)
∈𝑅
ℇ
=𝑒
,
𝑉
=𝟎
,𝟎
,ℇ
=𝑒
,
(2)
In Eq. (2), 𝐺
,
,
is a graph generated in the
temporal segment which corresponds to temporal
duration from Δ
to Δ
. If the current time instance
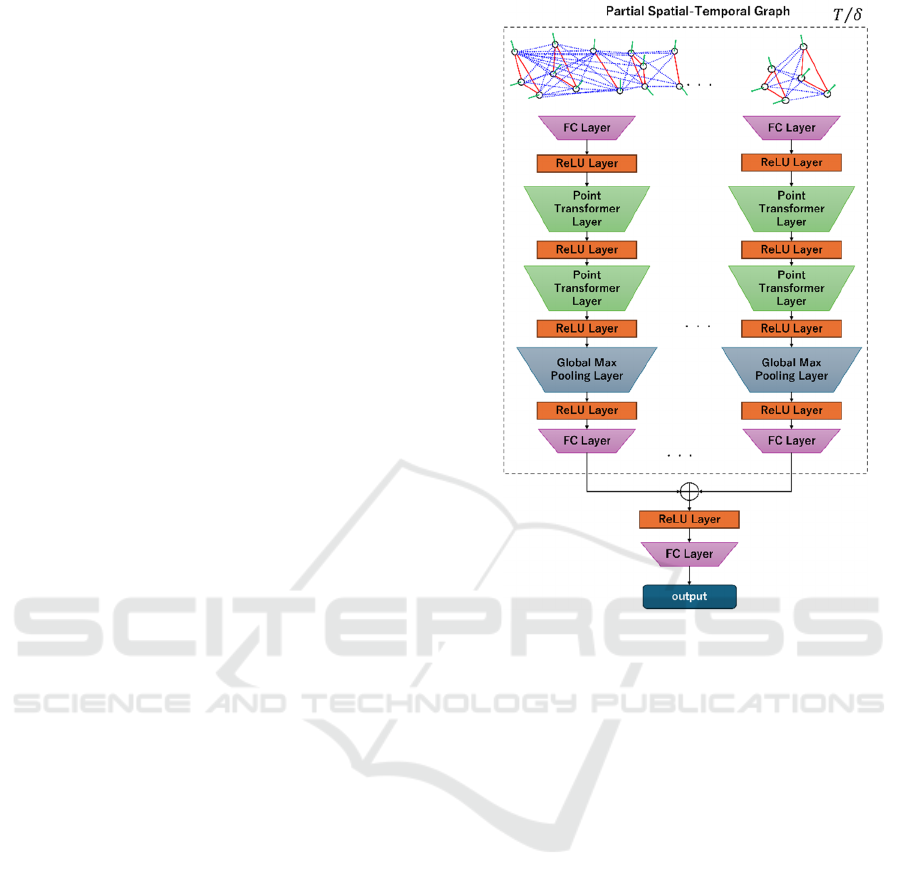
Figure 6: The structure of our model.
𝑡 is in the temporal segment, the graph is 𝑉
,ℇ
,
while the graph
(
𝑉
,ℇ
)
is the time instance 𝑡 is
before the start of Δ
. Similar to Eq. (1), 𝑉
,ℇ
is
the graph whose node contains the visual feature of
the bounding box surrounding the participant and the
position vector including the centroid coordinate of
the bounding box and the time instance. 𝑉
=
(𝟎
,𝟎
) has the zero vectors whose dimensions are
same as the visual feature and position vector,
respectively. ℇ
=𝑒
,
means self-connection of
only one node 𝑉
. The process of generating partial
spatial-temporal graph result in generating 𝑇/𝛿
graphs where 𝑇 is the length of entire duration and
𝛿= Δ
−Δ
is the length of each temporal segment.
By generating the spatial-temporal graph at each
segment, the local geometric feature can be preserved.
3.4 Graph Processing
After the partial spatial-temporal graph are acquired,
these graphs are input to our model. The input graphs
have the two aspects; graph and set of points with
visual features. Therefore, in this paper, the model
should be built based on the basic blocks which can
deal with these aspects.
A Group Activity Based Method for Early Recognition of Surgical Processes Using the Camera Observing Surgeries in an Operating Room
and Spatio-Temporal Graph Based Deep Learning Model
719

The model in our proposed method is shown in
Fig 6. The basic block is Point Transformer Layer
from (Zhao et al., 2021) which takes the point cloud
data as the input and deal with various task such as
classification, semantic segmentation and part
segmentation. Here, a brief review about point
transformer layer is shown.
In Point Transformer (Zhao et al., 2021), the self-
attention structure and position encoding are applied
to point cloud data which is a set of 3D points. The
processing in Point Transformer Layer is shown in Eq.
(3)
𝒙′
=𝜌(𝛾(𝜑
(
𝒙
)
−𝜓𝒙
+𝛿))
𝒙
∈()
⊙(𝛼𝒙
+𝛿)
(3)
In Eq. (3), 𝜒(𝑖) is a set of points which are connected
to 𝒙
which is feature of 𝑖-th point. 𝒙′
is the output of
Point Transformer Layer of 𝒙
. 𝜌 is a normalization
function. 𝛾 is a non-linear function. 𝜑, 𝜓 and 𝛼 are
functions for point wise transformation. 𝛿 is position
encoding function which is defined as below.
𝛿=𝜃(𝒑
−𝒑
)
(4)
In Eq. (4), 𝜃 is an encoding function. 𝒑
and 𝒑
are
the 𝑖-th and 𝑗-th position vectors, respectively.
As shown in Eq. (3) and (4), Point Transformer
Layer processes both the feature and position of the
point. The layer is used as building the block for
classification and segmentation of the point cloud.
Looking at our problem setting, our spatial-temporal
graph, which expand as time goes, can be treated as
the set of points with the visual features with the
variation of the shape. The reason is that the number,
position and actions of the participants vary over time.
Therefore, we apply Point Transformer Layer to deal
with our input graphs because the layer fits well to the
form of our input graph. Note the implementation of
the layer follows that of Pytorch Geometric (Pytorch
Geometric, 2024).
Our model has multi stream network structure so
that the local geometric structure of spatial-temporal
graph can be utilized in classification. Each stream
inputs the partial spatial-temporal graph from each
temporal segment. The multi stream extracts the
features from the graphs in the temporal segments
respectively. The last layer of each stream is global
max pool layer because the graph structure should be
represented in the form of a vector. The extracted
features from the streams are concatenated into one
vector. Finally, the concatenated vector is fed into the
small network for classification.
4 EXPERIMENTS
4.1 Dataset
To confirm the validity of our proposed method, we
conducted experiments on the publicly released
dataset called 4D-OR (Özsoy et al., 2022). The
dataset contains videos capturing mock surgery of
knee-replacement using multiple cameras. Using
each camera, 10 videos were acquired. The number
of participants is five. Note that our experiments do
not deal with the patient, which (Özsoy et al., 2022)’s
dataset includes; that is, our assumption is the patient
is not the member of the group.
Additionally, our method and (Zhai et al., 2023)
require bounding boxes surrounding the members of
the group in all frames because both (Zhai et al.,
2023) and our proposed method assume extracting the
visual features from local areas which surround the
participants in each frame. On the other hand, some
of surgical processes in 4D-OR (Özsoy et al., 2022)
have frames in which any of the participants does not
appear or in which detecting the participants
automatically is difficult even if the detection model
is well-finetuned. Therefore, the surgical processes in
which the participants always appear in all the frames
and are easy to be detected in each frame with object
detector such as (Liu et al., 2016) are chosen. For our
experiment, the video acquired by the second camera
of 4D-OR in the operating room is selected. The
contents of the surgical processes are shown in Table
1, where, if necessary, refer to (Özsoy et al., 2022) or
(Özsoy et al., 2024) for details of the dataset. The
average duration of each surgical process is computed
based on the number of the frames belonging to each
surgical process.
Table 1: The content and the average duration of each
surgical process.
Process Average duration # of instances
K
nee-
p
rep 01 min 56 sec 10
K
nee-inser
t
01 min 42 sec 10
P
atien
t
-
p
rep 02 min 55 sec 10
Surgery-
conclusion
01 min 28 sec 10
4.2 Conditions
For building our model, seven out of the ten videos
capturing surgeries are used for the training, one is
used for the validation, and the other two are used for
the test, where the one for validation is selected
randomly from the eight patterns after the two test
ICPRAM 2025 - 14th International Conference on Pattern Recognition Applications and Methods
720

(a) (b) ©
(d) (e) (f)
Figure 7: The examples of the images of [34] from surgical processes in which the passed durations are 1, 10 and 20 seconds.
The upper row shows the images of the process called surgery conclusion. The lower rows shows the images of the process
called patient-prep in which the passed durations are 1, 10 and 20 seconds.
patterns are removed. Therefore, the remaining seven
are used for training. The 45 test patterns are
examined in this paper.
For optimizing, Adam is used where the batch is
64.
In our experiments, the width and height of the
image are scaled to 1/8 of the original size of images
in (Özsoy et al., 2022). A machine used for
conducting our experiments is Ubuntu 20.04, AMD🄬
Ryzen 7 2700x eight-core processor x 16 and Nvidia
Geforce RTX 3060 which has one 12GB video card.
In this experiment, VGG16(Simonyan et al.,
2015) is used as the image feature extractor as shown
in Fig. 3. The extractor is not finetuned in advance to
train the entire model due to simplification of the
experiments.
In our experiments, it is assumed that the
participants are detected in images before both
training and inference. The participants are detected
by object detector SSD (Liu et al., 2016) which is
finetuned with frames sampled from all over the
dataset. For (Özsoy et al., 2022)’s dataset, in each
frame of the video, whether the number of detected
participants is equal to or less than the maximal
number of the participants is checked. If the number
of the detected participants is greater than the
maximal number of the participants, the detections
which do not comprise any of the participants are
removed because both previous work (Zhai et al.,
2023) and our proposed method assume extracting the
visual features from the local area (bounding box)
which comprises one participant in each frame. In
case of no detection despite of the fact that (a)
participant(s) is/are in the frame, the bounding
boxe(s) is/are placed manually.
For training the model, 20 epochs for 4D-OR
(Özsoy et al., 2022) are used. For training and
inference, the early observation is set to the duration
corresponding to from 1 to 30 seconds for all the
surgical processes. Note that each participant’s action
is not treated in both training and inference.
4.3 Results
The results of the early recognition on 4D-OR (Özsoy
et al., 2022) are shown in Table 2 respectively. Using
the F-value of each process in each test, the means,
and standard deviations of F-values all over the test
patterns are computed.
Table 2: The f-value at each process of 4D-OR (Özsoy et
al., 2022).
Process Mean and standard deviation of F-value
Knee-prep
0.787 +
/
- 0.193
Knee- insert
0.852 +
/
- 0.104
Patient-prep
0.900 +
/
- 0.141
Surgery-
conclusion
0.682 +/- 0.230
In this paper, the comparison with state of the art
in terms of early recognition of the group activity is
conducted to confirm the superiority of our proposed
method. While there are two major conventional
A Group Activity Based Method for Early Recognition of Surgical Processes Using the Camera Observing Surgeries in an Operating Room
and Spatio-Temporal Graph Based Deep Learning Model
721

works (Chen et al., 2020), and (Zhai et al., 2023) as
stated in Sec 2, in this paper, (Zhai et al., 2023) is
chosen for this comparison because (Zhai et al., 2023)
is state of the art among the major works of group
activity based early recognition and their codes are
publicly released. For this comparison the method
proposed by (Zhai et al., 2023) is implemented based
on the available code and modified so that the dataset
can be examined. Note that (Zhai et al., 2023) ‘s
visual feature extractor is finetuned in advance to
training the entire model.
The results shown in Table 3, in which F-value are
listed. The bounding boxes surrounding the
participants are detected by SSD (Liu et al., 2016),
which is finetuned based on the datasets used in this
paper respectively. For training and inference, the
early observation is set to temporal lengths
corresponding to from 1 to 30 seconds for all the
surgical processes.
Table 3: The comparison with (Zhai et al., 2023) at each
process of 4D-OR (Özsoy et al., 2022).
Process (Zhai et al., 2023) Ours
Knee- prep
0.653 +
/
- 0.260 0.787 +
/
- 0.193
Knee-insert
0.715 +
/
- 0.193 0.852 +
/
- 0.104
Patient-prep
0.907 +
/
- 0.133 0.900 +
/
- 0.141
Surgery-
conclusion
0.636 +/- 0.234 0.682 +/- 0.230
5 DISCUSSIONS
5.1 Contribution and Limitations
As shown in Table 2, the F values is 68.2% at least
based on the observed frames until 30 seconds from
the beginning, which correspond to 34.1 %
observation in surgery conclusion. Furthermore, the F
values in knee-prep, knee-insert and patient-prep are
more than 75% which is relatively high value. These
results mean our model can recognize these surgical
processes based on the video frames which are
observed until 30 seconds. In terms of observation
ratio, if 25.9% (almost equals to 30 secs / 1 min 56
secs), 29.4% (almost equals to 30 secs / 1 min 42 secs)
and 17.1% (almost equals to 30 secs / 2 min 55 secs)
observed information is obtained, our model can
recognize these surgical processes. The important
element of this successful performance seems to
derive from representation of the input and the model
design. In terms of the representation of the input, the
spatial-temporal graph contains not only the visual
features but also the position and the number of the
participants and their temporal variation. Furthermore,
in our input graph, the temporal variation of the
position and the number of the participants is a
geometric shape in spatial-temporal space. For
example, if the number of participants changes from
three to two, the number of vertices decreases. In the
perspective of geometric shape, the shape of the point
set is sharpened. The shape in spatial-temporal space
can be distinguishable cue in early stage at high
accuracy. In terms of model design, using Point
Transformer Layer which can treat both the feature
and position of the points fit to our input graph data.
On the other hand, the F-value at surgery-
conclusion is lower than those of other processes.
This comes from the similarity in terms of the shape
of the graph in spatial-temporal space. Looking at the
frames of surgery conclusion until 30 seconds, the
position and number of participants seem to be
similar to other processes for example the patient-
prep until 20 seconds. As time passes, the unique cues
come to appear in the video frames. The cues are for
example that the surgeons get out of the room and
remained assistants start to clear the instruments.
However, our method seems to fail to capture this
detailed cue. One of the possibilities of the failure lies
in how to make the temporal segments for generating
partial spatial-temporal graph. Although we took the
strategy which divides the temporal duration to make
multiple spatial-temporal graphs so that the shape
feature of the graph can be preserved, it may be
difficult to capture the local shape for our model if the
granularity of the division of temporal segments is
coarse. Therefore, how to divide the temporal
segments for generating optimal graph from other
processes should be researched as future work.
5.2 Comparison to the State of the Art
Table 3 shows that our proposed method performs
better or competitive compared to (Zhai et al., 2023).
In particular, our proposed method outperforms (Zhai
et al., 2023) in the recognition of knee-prep and knee-
insert significantly. The reason seems to be that our
method treats not only the visual features of the
participants but also the positions and the number of
those by representing them as the shape of the graph,
while (Zhai et al., 2023) treats only the visual features
of the participants by merging them via pooling.
6 CONCLUSIONS
This paper has proposed a group activity-based
method for early recognition of surgical processes
using the camera attached to the ceiling of the
ICPRAM 2025 - 14th International Conference on Pattern Recognition Applications and Methods
722

operating. To deal with this problem setting, the
proposed method (1) makes the spatial-temporal
graphs which represents not only visual features of
the participants but also the positions and the number
of the participants and (2) uses the graph to classify
to the category of the surgical processes. Our model
utilizes Point Transformer Layer as the building
blocks to deal with the graphs which has the
geometric information in spatial-temporal space.
By using the model, the early recognition of the
surgical process is performed on the public datasets;
mock surgery of knee replacement (Özsoy et al.,
2022). Experimental results show that our method can
recognize each surgical process from early durations
of the inputted video, where the F1 values in the
public dataset (Özsoy et al., 2022) are from 68.2% to
90.0% in 30 seconds from the beginning. These
results mean our method can recognize the surgical
process based on from early part 17.1 % to 34.1 % of
the entire information in (Özsoy et al., 2022),
respectively. Compared with the state-of-the-art in
terms of early recognition for the group activity (Zhai
et al., 2023), it is shown that that ours outperforms
(Zhai et al., 2023) in 4D-OR dataset (Özsoy et al.,
2022).
REFERENCES
Y. Li, J Ohya, T. Chiba, R. Xu, H. Yamashita (2016). ”
Subaction Based Early Recognition of Surgeons' Hand
Actions from Continuous Surgery Videos”, IIEEJ
Transactions on Image Electronics and Visual
Computing Vol.4 No.2
H Zhao, P. Wildes (2021). ” Review of Video Predictive
Understanding: Early Action Recognition and Future
Action Prediction”, arXiv:2107.05140v2.
B. Zhou, A. Andonian, A. Oliva, A. Torralba (2018). ”
Temporal Relational Reasoning in Videos”,
arXiv:1711.08496
L. Chen, J. Lu, Z. Song, J Zhou (2018). ” Part-Activated
Deep Reinforcement Learning for Action Prediction”,
Proc. of ECCV, pp 435–451.
G. Singh, S. Saha, M. Sapienza, P. Torr, F. Cuzzolin (2017).
” Online Real-Time Multiple Spatiotemporal Action
Localisation and Prediction”, Proc of ICCV, pp. 3657–
3666
C. Sun, A. Shrivastava, C. Vondrick, R. Sukthankar, K.
Murphy, C. Schmid (2019). ” Relational Action
Forecasting”, Proc of CVPR, pp. 273–283
S. Ma, L. Sigal, S. Sclaroff: (2016). ”Learning Activity
Progression in LSTMs for Activity Detection and Early
Detection”, Proc of CVPR, pp.1942–1950
M. S. Aliakbarian, F. S. Saleh, M. Salzmann, B. Fernando,
L. Petersson, L. Andersson (2017). ” Encouraging
LSTM to Anticipate Actions Very Early”,
arXiv:1703.07023
Y. Kong, Z. Tao, Y. Fu (2017). ” Deep Sequential Context
Networks for Action Prediction”, Proc of CVPR,
pp.3662–3670
Y. Kong, D. Kit, Y. Fu (2014). ”A Discriminative Model
with Multiple Temporal Scales for Action Prediction”,
Proc of ECCV, pp. 596–611
X. Wang, J. Hu, J. Lai, J. Zhang, W. Zheng (2019).
”Progressive Teacher-Student Learning for Early
Action Prediction”. Proc of CVPR, pp. 3551–3560.
J. Bradbury, S. Merity, C. Xiong, R. Socher (2016). “Quasi-
Recurrent Neural Networks”, arXiv:1611.01576v2
H Zhao, R. Wildes (2019). ”Spatiotemporal Feature
Residual Propagation for Action Prediction”, Proc of
ICCV, pp. 7002–7011
K. Soomro, A. R. Zamir, M. Shah (2012). “UCF101: A
Dataset of 101 Human Actions Classes From Videos in
The Wild”, arXiv:1212.0402
H. Jhuang, J. Gall, S. Zuffi, C. Schmid, M. J. Black (2013).
“Towards Understanding Action Recognition”, Proc of
ICCV, pp. 3192–3199
Y. Kong, Y. Jia, Y. Fu (2012). ”Learning Human
Interaction by Interactive Phrases”, Proc of ECCV, pp.
300–313,
A. Patron-Perez, M. Marszalek, A. Zisserman, I. Reid:
“High Five: Recognising human interactions in TV
shows”, Proc of BMVC, pp. 50.1–50.11, (2010)
(doi:10.5244/C.24.50)
R. Goyal et al. (2017). “The “Something Something” Video
Database for Learning and Evaluating Visual Common
Sense”, Proc of ICCV, pp. 5843– 5851
J. Hu, W. Zheng, J. Lai, J. Zhang (2017). “Jointly Learning
Heterogeneous Features for RGB-D Activity
Recognition”. TPAMI, vol.39, no.11, pp.2186-2200
Y. Li, C. Lan, J. Xing, W. Zeng, C. Yuan, J. Liu (2016).
”Online Human Action Detection Using Joint
Classification-Regression Recurrent Neural
Networks”, proc of ECCV, pp. 203–220
C. Liu, Y. Hu, Y. Li, S. Song, J. Liu (2017). “PKU-MMD:
A Large Scale Benchmark for Continuous Multi-Modal
Human Action Understanding”, arXiv:1703.07475
K.Simonyan, A.Zisserman, (2015). “Very Deep
Convolutional Networks for LargeScale Image
Recognition”, arXiv:1409.1556v6,
J. Chen, W. Bao, Y. Kong: Group Activity Prediction with
Sequential 14 Relational Anticipation Model,
arXiv:2008.02441v1 (2020)
The Japan Institute for Labour Policy and Training (2022).
https://www.jil.go.jp/kokunai/blt/backnumber/2022/11
/s_02.html access 2023/04/
M Ibrahim, et al. (2016) “A Hierarchical Deep Temporal
Model for Group Activity Recognition”,
arXiv:1511.06040
W. Choi, K. Shahid, S. Savarese, (2009). “What are they
doing? : Collective Activity Classification Using
Spatio-Temporal Relationship Among People.” 9th
International Workshop on Visual Surveillance
(VSWS09) in conjuction with ICCV,
https://cvgl.stanford.edu/projects/collective/collective
Activity.html
A Group Activity Based Method for Early Recognition of Surgical Processes Using the Camera Observing Surgeries in an Operating Room
and Spatio-Temporal Graph Based Deep Learning Model
723

W.Liu et al., (2016) “SSD: Single Shot MultiBox Detector”,
arXiv:1512.02325
X. Zhai et al. (2023). "Learning Group Residual
Representation for Group Activity Prediction*," 2023
IEEE International Conference on Multimedia and
Expo (ICME), Brisbane, Australia, pp. 300-305,
K. Yokoyama et al. (2023). “Operating Room Surveillance
Video Analysis for Group Activity Recognition,”
Advanced Biomedical Engineering, vol.12, p.171-181,
E. Özsoy et al., “4D-OR: Semantic Scene Graphs for OR
Domain Modeling”, arXiv:2203.11937
E. Özsoy et al., (2024). “Holistic OR domain modeling: a
semantic scene graph approach”, Int J CARS 19, 791–
799.
A. Shargi et al. (2020). “Automatic Operating Room
Surgical Activity Recognition for Robot-Assisted
Surgery”, arXiv:2006.16166
L. Bastian et al. (2022), “Know your sensORs -- A Modality
Study For Surgical Action Classification”,
arXiv:2203.08674
J. Wu et al. (2019). “Learning Actor Relation Graphs for
Group Activity Recognition”, arXiv:1904.10117
S. Li et al. (2021). “GroupFormer: Group Activity
Recognition with Clustered Spatial-Temporal
Transformer”, arXiv:2108.12630
Microsoft (2021). https://learn.microsoft.com/ja-jp/previo
us-versions/azure/kinect-dk/hardware-specification#de
pth-camera-supported-operating-modes accessed at
2024/09/08
H. Zhao et. al, (2021) “Point Transformer”,
arXiv:2012.09164
Pytorch Geometric (2024) PyG Documentation —
pytorch_geometric documentation (access 2024/11/13)
K. He et al., (2017), Mask-RCNN, arXiv:1703.06870
ICPRAM 2025 - 14th International Conference on Pattern Recognition Applications and Methods
724
