
Cyber Threat Modeling of an LLM-Based Healthcare System
Neha Nagaraja
1 a
and Hayretdin Bahsi
1,2 b
1
School of Informatics, Computing, and Cyber Systems, Northern Arizona University, Flagstaff, U.S.A.
2
Department of Software Science, Tallinn University of Technology, Tallinn, Estonia
Keywords:
Healthcare, Large Language Models, Cyber Threats, Conversational Attacks, Adversarial Attacks, Threat
Modeling.
Abstract:
With the rapid advancement of large language models (LLMs) and their integration into the healthcare sys-
tem, it is critical to understand their resiliency against cyber-attacks since sensitive data handling is paramount.
Threat modeling is most important, as addressing cybersecurity early in system development is essential for
safe and reliable deployment. While traditional threat modeling practices are well-established, applying these
frameworks to systems integrating LLM, especially in healthcare, presents unique challenges. It is essential
to examine conventional cyber threats, adversarial threats, and threats specific to LLM in tandem to build
robust defense mechanisms. This paper adapts the STRIDE methodology to assess threats in LLM-powered
healthcare systems holistically, identifying components and their data flows and mapping potential threats in-
troduced by each component. It provides practical guidance for understanding the threats early in development
and demonstrates effective system modeling tailored to healthcare settings.
1 INTRODUCTION
Large Language Models (LLMs), such as GPT-4
(OpenAI), LLaMA (Meta), and Bard (Google), have
revolutionized natural language processing by set-
ting new benchmarks in generating human-like text,
driving advancements in fields such as conversa-
tional agents, content automation, and data analysis
for decision-making systems (Chu et al., 2024)(Shah
et al., 2024). The widespread accessibility of these
models via user-friendly platforms, such as chatbots
and APIs, has enabled various industries to leverage
sophisticated language processing without the need
for specialized expertise (Abbasian et al., 2024)(Deng
et al., 2024). In healthcare, LLMs have signifi-
cantly enhanced medical information retrieval, pa-
tient communication, diagnostic support, and person-
alized treatment recommendations (Abbasian et al.,
2024)(Tang et al., 2024).
However, integrating LLMs into healthcare sys-
tems introduces significant ethical and cybersecurity
challenges that must be carefully addressed (Panka-
jakshan et al., 2024). Recent studies have high-
lighted various threats associated with LLMs, includ-
ing prompt injection attacks, jailbreak methods, data
a
https://orcid.org/0009-0000-2967-244X
b
https://orcid.org/0000-0001-8882-4095
contamination, and the generation of misinformation,
all of which exacerbate these risks and necessitate ad-
vanced defense mechanisms (Chu et al., 2024)(Path-
manathan et al., 2024)(Balloccu et al., 2024). These
threats can pose significant risks, including the spread
of false medical advice, breaches of sensitive patient
data, and a loss of trust in healthcare systems (Brown
et al., 2024)(Greshake et al., 2023). The poten-
tial for LLMs to generate and propagate misinforma-
tion adds another layer of complexity, particularly in
healthcare, where accurate information is paramount
(Shah et al., 2024). While LLMs offer transfor-
mative potential for the healthcare sector (Abbasian
et al., 2024), their integration must be accompanied
by robust threat modeling and comprehensive security
measures. Threat modeling is a crucial early-stage ac-
tivity in the secure development lifecycle (SDLC), en-
abling the identification and assessment of potential
risks. By systematically categorizing and addressing
threats, we can implement adequate safeguards that
protect both the integrity of healthcare systems and
the well-being of patients.
Attacks on the conversational interfaces of LLMs
(e.g., prompt injection, jailbreaks) have recently
drawn significant interest within research communi-
ties. LLMs can also be targeted by attacks (e.g.,
model inversion, model extraction) inherited from the
Nagaraja, N. and Bahsi, H.
Cyber Threat Modeling of an LLM-Based Healthcare System.
DOI: 10.5220/0013289700003899
In Proceedings of the 11th International Conference on Information Systems Security and Privacy (ICISSP 2025) - Volume 1, pages 325-336
ISBN: 978-989-758-735-1; ISSN: 2184-4356
Copyright © 2025 by Paper published under CC license (CC BY-NC-ND 4.0)
325

adversarial machine learning security domain. As
LLMs are part of integrated systems in real-world im-
plementations, threat actors can resort to conventional
cyber threats (e.g., eavesdropping, denial of service)
against the attack surfaces. Threat actors can combine
various threat types in a single attack campaign. Thus,
it is imperative to have a holistic understanding of all
three threat landscapes in a unified threat modeling
framework. Such a perspective has not been reflected
in existing threat modeling studies.
This paper demonstrates how the widely used
STRIDE threat modeling approach can be adapted to
systems with LLM-based components. Specifically,
we illustrate an LLM-based system using a data flow
diagram (DFD) for a healthcare system case study.
We then identify security boundaries and systemati-
cally elicit threats relevant to the system, focusing on
adversarial, conversational, and conventional threats.
The unique contribution lies in our detailed demon-
stration of system modeling for the LLM-based case
study and systematic threat elicitation, integrating
both the LLM and cybersecurity perspectives.
Despite the importance of threat modeling, there
is a notable scarcity of research focusing on LLM-
based systems. This is especially true for studies ad-
dressing system modeling and systematic threat elici-
tation. Effective threat modeling for LLM-integrated
healthcare systems necessitates combining conven-
tional, adversarial, and LLM-specific conversational
threats. Our paper addresses this research gap by of-
fering a structured approach to threat modeling that
considers the unique challenges posed by LLMs in
healthcare. By doing so, we provide a valuable frame-
work for securing LLM-integrated systems, an area
that remains underexplored in the current literature.
The paper is organized as follows: Section 2 re-
views related work, Section 3 outlines the study’s
methodology, Section 4 presents the case study re-
sults, Section 5 discusses key findings, and Section
6 concludes the paper.
2 RELATED WORK
Research on large language model security and ro-
bustness has rapidly advanced, uncovering a wide
range of vulnerabilities that threaten their safe usage
across various domains. Attacks such as prompt in-
jections—jailbreaks have been a focus as adversaries
manipulate inputs to elicit malicious outputs from the
models. Many studies have classified and compre-
hensively evaluated how these attacks are applied so
that even minimal manipulations can induce harmful
behaviors (Chu et al., 2024)(Deng et al., 2024)(Gre-
shake et al., 2023)(Rossi et al., 2024). In addition, the
integration of third-party LLM plugins and APIs in
the application raises new vulnerabilities, such as pro-
prietary information leakage and malicious exploita-
tion (Iqbal et al., 2024)(Zhao et al., 2024)(Finlayson
et al., 2024). Data contamination is a critical threat
resulting from the manipulation of training data, lead-
ing to degraded model performance and enabling the
extraction of proprietary knowledge without access to
the original dataset (Pathmanathan et al., 2024)(Bal-
loccu et al., 2024)(Truong et al., 2021).
In healthcare, LLMs are used for tasks like medi-
cal knowledge retrieval and personalization of treat-
ments (Abbasian et al., 2024)(Tang et al., 2024),
but their strengths also make them easy to misuse,
such as spreading false medical advice, misinforma-
tion, or unauthorized access to sensitive patient data
(Shah et al., 2024)(Chen and Shu, 2024). Stud-
ies have shown that sophisticated attack vectors like
indirect prompt injection can remotely compromise
LLM-integrated healthcare applications, leading to
severe consequences such as data breaches and the
undermining of trust in medical systems (Chu et al.,
2024)(Greshake et al., 2023).
To mitigate these threats, frameworks such as
STRIDE (Tete, 2024) and risk assessments (Panka-
jakshan et al., 2024) are used to identify and evaluate
risks. However, despite using STRIDE & DREAD,
Tete’s framework focuses on high-level threat iden-
tification without linking threats to specific system
components (Tete, 2024). Similarly, Pankajakshan et
al. emphasize broad risk categorization across stake-
holders but lack detailed, component-specific threat
elicitation (Pankajakshan et al., 2024). Both ap-
proaches fail to provide the structured system mod-
eling needed to identify which components introduce
specific threats, limiting their effectiveness for tar-
geted security measures.
The categorization of LLM threats is provided by
resources such as MITRE ATLAS (MITRE, 2024),
the OWASP Top 10 LLM threats (OWASP, 2024),
and NIST Adversarial ML (Vassilev et al., 2023).
These frameworks highlight the importance of align-
ing LLMs with human values & adhering to regu-
latory standards, such as the European Union’s AI
Act and the NIST AI Risk Management Framework,
to ensure ethical & secure deployment (Tang et al.,
2024). These resources are instrumental knowledge
bases for threat modeling.
Our paper uniquely advances the field by focusing
on structured system modeling and systematic threat
elicitation, pinpointing which components generate
specific threats. Unlike prior studies, we comprehen-
sively address common cyberattack vectors, adversar-
ICISSP 2025 - 11th International Conference on Information Systems Security and Privacy
326

ial threats, and conversational threats within a unified
threat assessment framework, providing a holistic, ac-
tionable guide for secure LLM deployment.
3 METHODS
In this section, we outline the approach taken to iden-
tify and address potential security threats within our
LLM-based healthcare system. The objectives em-
ployed in this study are defined in the security objec-
tives. We next defined our system and its components
in the system modeling phase and then conducted a
comprehensive threat elicitation. By establishing a
clear attack taxonomy, we aim to systematically cate-
gorize potential threats for each component.
3.1 Security Objectives
Our study aims to identify potential threats in a
healthcare system integrated with large language
models (LLMs). We are focused on protecting tradi-
tional and LLM-specific threats to ensure the system’s
CIA Triad—confidentiality, integrity, and availability.
We have categorized threats into three main types:
(1) Conventional Cyber Threats — These are typ-
ical cyber threats that mainly target the infrastructure
and core system components, compromising the con-
fidentiality, integrity, and availability of the systems,
such as MiTM attacks, unauthorized access, malware,
or denial of service. In our system, unauthorized ac-
cess to healthcare data & patient information is criti-
cal due to the sensitive nature of the data and the im-
portance of regulatory compliance (e.g., HIPAA).
(2) Adversarial Threats — These threats specif-
ically target the machine learning models (Papernot
et al., 2018). As our system incorporates differ-
ent models to provide decision-making support, these
threats can compromise the behavior and performance
of the models. These attacks include inference at-
tacks, model extraction, model evasion, and so on
(Vassilev et al., 2023). In our system, attackers might
first exploit traditional cyber threats to access critical
assets (e.g. bypassing web applications, firewalls, or
APIs) before executing adverse attacks on the models.
(3) Conversational Threats — These threats
specifically target interactions between user input and
external sources that feed into the LLM. Such threats
compromise the integrity of LLM outputs by manip-
ulating the model’s operation or behavior. We intro-
duce this additional category to distinguish between
general adversarial threats and the more specific at-
tacks that exploit conversational interfaces. These at-
tacks often manifest through direct or indirect prompt
injections (OWASP, 2024).
Given this context, our specific security assump-
tions include:
1) In this paper, we rely on third-party LLMs. We
do not have direct control over their training process
or data assets. Therefore, the risk of training data poi-
soning attacks falls within the scope of the Service-
level agreements (SLAs) with third-party providers
and is not a concern in this study. Instead, we focus
on risks that we can manage and control.
2) Fine-tuning of the LLMs is considered out-
side the scope of our current objectives. Hence, any
risks like data leakage or adversarial manipulation are
eliminated. Our focus is solely on the secure use of
pre-trained models provided by third-party vendors.
3) We aim to uphold the intellectual property
rights of the third-party LLMs used in our system.
In the scope of the study, we do not provide com-
plete privacy threat modeling. Instead, we focus on
the security threat model of the LLM-based system
architecture. Although our model identifies various
privacy risks, it does not address all privacy concerns,
such as linkability or identifiability. Privacy-centric
analysis requires frameworks similar to LINDDUN
(Deng et al., 2011).
3.2 System Modeling
We perform system modeling to better understand the
complex interactions within a system. In this study,
we have adopted a Level 1 Data Flow Diagram (DFD)
to model the system, breaking down the process into
sub-processes and illustrating data flows and stores.
There are three ways of incorporating LLMs into
any system (I. S. Authority, 2024) - (1) Integrating
LLM via API provided by an external provider (Ope-
nAI, Anthropic). (2) Importing a pre-trained LLM
(open-source or third-party like Mistral) with an op-
tion of further fine-tuning. (3) The organization de-
signs, trains, and deploys its own LLM (in-house
LLM). In this study, we follow the second approach
by using a pre-trained model without fine-tuning.
To assess potential threats, we have utilized the
STRIDE framework (Spoofing, Tampering, Repudia-
tion, Information Disclosure, Denial of Service, and
Elevation of Privilege), which is applied to the DFD
elements as shown in the table below. The threats
were mainly identified based on the attack taxonomy.
We designed our DFD based on a conversational
health agent called openCHA, an open-source frame-
work with a large language model (LLM) accessed
via API (Abbasian et al., 2024). However, in our
study, we have opted for Option 2—importing a
pre-trained LLM from a third-party or open-source
Cyber Threat Modeling of an LLM-Based Healthcare System
327
Table 1: STRIDE-per-Element: Applicable Threats to DFD
Elements (Shostack, 2014).
DFD Element S T R I D E
Entity ✓ ✓
Process ✓ ✓ ✓ ✓ ✓ ✓
Data Flow ✓ ✓ ✓
Data Store ✓ ✓ ✓ ✓
provider (e.g., Mistral) to have better control over
data. We do not fine-tune the model; instead, we use
it as-is and deploy it within our infrastructure. By do-
ing so, we ensure that sensitive healthcare data is pro-
cessed securely without relying on external API calls
from third-party providers.
The system is divided into five major components:
Web Application, Healthcare Platform, Orchestrator,
External Sources and LLM, as illustrated in Figure 1.
In the openCHA, as described by Abbasian et al.
(2024), the Orchestrator consists of the Task Execu-
tor, Task Planner, Prompt List, Response Generator,
and Data Pipe. For simplicity, we have combined the
roles of the Prompt List with the Task Executor and
the Response Generator with the Task Planner.
Unlike the original openCHA framework, where
Healthcare Platforms were treated as external re-
sources, we’ve chosen to integrate the Healthcare
Platform directly into our system. This is because it
holds crucial patient information that needs to remain
secure and cannot be exposed to outside entities. By
including it within the system boundary, we can bet-
ter protect sensitive patient data and ensure that it is
handled with care. Using these data, we can generate
a more personalized response.
To effectively manage and maintain the LLM, we
have divided its life cycle (IBM, 2024) (Shi et al.,
2024) into three primary stages: The first stage in-
volves model deployment and versioning, ensuring
seamless integration and updates. The second stage
is the LLM process, which handles queries and gen-
erates responses, followed by the third stage, which
focuses on performance metrics, monitoring, and log-
ging to ensure accuracy, efficiency, and compliance.
While designing our DFD diagram, we were de-
termined to depict each component accurately. When
deciding whether to represent the LLM component as
a data store or a process, we considered several fac-
tors - (1) Its role in the system. (2) The level of con-
trol we have over it, (3) how well it fits within the
architecture. Since the LLM plays an active role in
processing user inputs, generating strategies, and in-
teracting with components like the Task Planner com-
bined with the level of control, we have over LLM’s
operations and determined that LLM functions as a
process rather than a data store.
From the STRIDE perspective, if we treat LLM as
a data store, the primary threats would be T, R, I, and
D. However, it is essential to account for S and E, as
LLM could be spoofed by an attacker impersonating
all legitimate entries, leading to malicious or incorrect
inputs being processed. If the system misconfigures
access controls, the LLM could gain elevated privi-
leges, allowing unauthorized access to sensitive data
or critical system actions.
We have represented the third-party repository as
an entity in our system because it is an external re-
source over which we have no direct control. Our
main concerns are Spoofing (ensuring we receive up-
dates from a legitimate source) and Repudiation (veri-
fying and tracking the receipt of updates). T, I, D, and
E threats against these repositories are not concerns in
our study (handled by SLAs) as we do not alter, ac-
cess sensitive information, or manage the repository’s
operations. However, the information flow between
the external resource and our system is subject to var-
ious threats (e.g., eavesdropping or MiTM) that we
consider in this study.
The data flow from the Third-Party Repository
(entity) to the Model Deployment & Versioning (pro-
cess) represents periodic updates or new versions re-
ceived by our system. The third-party repository is
external to our system and we have no direct control
over it. All version information and updates are stored
in the data store called the model store. It is essential
to continuously track and evaluate LLM performance,
such as speed and resource utilization, and track logs
to identify bottlenecks, ensure transparency, and pro-
vide audit material, which is extremely important in
healthcare. This is done using the Performance met-
rics and Monitoring process shown in our DFD. These
performance data and inference logs are stored in the
Metrics & Logs store (data store).
In Section 4.1, we will dive deeper into the sys-
tem’s data flows, explaining how each component
works together.
3.3 Security Boundaries
In STRIDE, security or trust boundaries are defined
as the borders between different trusted zones within
the system. They are crucial for identifying areas
where potential security risks may arise. The bound-
aries are drawn based on the system’s attack surface
to reflect where potential malicious interactions could
occur. During threat elicitation, any components de-
fined within a trust boundary are considered trusted
and generally excluded from direct analysis. All data
flows that cross these boundaries are suspected and
must be thoroughly analyzed as they present a higher
ICISSP 2025 - 11th International Conference on Information Systems Security and Privacy
328

risk. More details on the security boundaries and their
impact on our Threat Modeling process are explained
in Section 4.2.
3.4 Threat Elicitation
Before we delve into threat elicitation, it is crucial to
establish a comprehensive attack taxonomy. This will
provide a clear framework for understanding the vari-
ous potential threats and serve as a foundation for the
subsequent analysis.
Attack Taxonomy. We have utilized the MITRE
ATLAS framework in our attack taxonomy, extend-
ing it with specific threats from the OWASP Top 10
for LLM applications and traditional cybersecurity
threats. This comprehensive approach ensures that
general cybersecurity and LLM-specific threats are
addressed, which is especially crucial in all domains,
including healthcare.
The mapping between OWASP and MITRE AT-
LAS demonstrates that several OWASP-identified
threats align directly with corresponding MITRE AT-
LAS entries. For instance, LLM01 (Prompt Injection)
corresponds to MITRE ATLAS’s LLM Prompt Injec-
tion, LLM03 (Training Data Poisoning) maps to Poi-
soning Training Data, LLM04 (Model Denial of Ser-
vice) to Denial of ML Service, LLM05 (Supply Chain
Vulnerabilities) to ML Supply Chain Compromise,
LLM06 (Sensitive Information Disclosure) to LLM
Data Leakage, LLM07 (Insecure Plugin Design) to
LLM Plugin Compromise, and LLM10 (Model Theft)
to Extract ML Model (MITRE, 2024) (OWASP,
2024). However, some OWASP threats, specifically
LLM02 (Insecure Output Handling), LLM08 (Exces-
sive Agency), and LLM09 (Overreliance) do not have
direct equivalents in the MITRE ATLAS framework.
Of these, LLM09: Overreliance is considered out
of scope for our study since we are not focusing on the
hallucination of LLMs, and we assume the LLM out-
puts to be trustworthy. Therefore, to create a compre-
hensive attack taxonomy for our system, we have ex-
tended the MITRE ATLAS framework to include two
additional threats from OWASP: LLM02: Insecure
Output Handling and LLM08: Excessive Agency. In
addition, we have considered traditional cybersecu-
rity threats to grasp the complete threat modeling. We
acknowledge that as the number of LLM applications
in healthcare grows, new vulnerabilities may develop,
demanding constant updates.
In this study, we use STRIDE-per-element rather
than STRIDE-per-interaction to systematically iden-
tify threats for each system component, considering
specific attack methods, preconditions, and mitiga-
tions (Shostack, 2014). This structured approach im-
proves clarity in mapping threats to DFD compo-
nents, such as entities, data stores, processes, and data
flows. In section 4.3, we will delve deeper into the
specifics of our threat modeling process, providing a
detailed analysis of how we applied the STRIDE-per-
element methodology across different components of
our healthcare system.
4 RESULTS
4.1 System Modeling
The DFD in Figure 1 describes the entire system. We
identified five entities, thirty-three data flows, seven
processes, and four data stores. The User ( i.e., pa-
tient or any healthcare provider such as a doctor) is
considered an entity in our system. We have divided
the system into five major components:
Web Application: The Web application serves as
the user interface, allowing users to input natural lan-
guage queries and ensuring secure data transmission
between the user and the system.
Healthcare Platform: This (process) stores sen-
sitive patient health records in the Patient Database
(data store). It interacts with the Web Application and
the Task Executor to provide patient data, which can
be either presented to the User or used for a personal-
ized response.
Orchestrator: As described by Abbasian et al.
(2024), the Orchestrator is one of the system’s core
components. We divided it into Task Executor (pro-
cess); Task Planner (process); and Data Pipeline (data
store). The Task Executor is responsible for convert-
ing and processing user queries and extracting the
necessary information; it also interacts with external
resources. It plays a central role in managing the
workflow within the system. It sends user queries
and relevant data to the Task Planner to generate
strategies and responses. It also requests the Health-
care Provider and gets the patient data sent to the
Task Planner for a personalized response. It interacts
with External Resources to get translated text clinical
knowledge data and ai/ml analyzed patient insights.
The Task Planner is the decision-making component
of the system. It analyzes user queries, formulates a
strategy, and divides the tasks required to generate a
response. It works with the LLM to refine the strategy
and develop a personalized response. It also sends the
relevant instructions to the Task Executor for execu-
tion. All intermediate data from these instructions and
analyzed patient insights and user prompts are stored
in the Data Pipeline which is a repository that man-
ages metadata from external sources and data gener-
Cyber Threat Modeling of an LLM-Based Healthcare System
329

ated during task execution. This information is crucial
in multi-step process thinking and is available to the
Task Executor and the Task Planner.
External Resources: As described by Abbasian et
al. (2024), these are external entities that provide the
system with additional data, insights, knowledge, and
translation capabilities. We have considered a Trans-
lator, Knowledge Base, and AI & Analysis Models as
our external resources for this system. Each of these
resources is accessed via API by the Task Executor.
If a user’s inputs are non-English, the Task Executor
sends a translation request to the Translator, which
converts the query into English, supporting multiple
languages in the system. The Knowledge Base re-
trieves up-to-date information from trusted healthcare
sources to prevent bias or hallucination in LLM re-
sponses. The AI & Analysis Models leverage analyt-
ics tools to derive insights, complementing LLMs to
enhance data processing and inference capabilities.
Large Language Model Component: This core
component is responsible for processing natural lan-
guage input, understanding context, and generat-
ing appropriate responses based on user queries and
healthcare data. We have further divided this into
three lifecycle stages (IBM, 2024) (Shi et al., 2024)
of the LLM. First is Model Deployment & Version-
ing, which is represented as a process responsible
for the deployment and versioning of models, ensur-
ing the system uses the latest and most secure ver-
sions. A Third-party Repository, identified as an en-
tity, provides all these model versions stored in the
Model Store, which is considered a data store. The
data flow between the deployment process and the
repository is infrequent and periodic, as it periodi-
cally retrieves model weights and updates from the
repository to keep the LLM current. The Model Store
also maintains version information, ensuring that the
correct model is used for processing queries. Sec-
ond is the LLM model, which receives structured
prompts and data from the Task Planner to gener-
ate strategies and responses. These responses are
then sent back for further processing, continuing in a
bidirectional data flow until a satisfactory outcome is
achieved. Lastly, Performance and Monitoring (pro-
cess) monitors the system’s performance, logs data,
and maintains records to ensure the LLM’s accuracy,
efficiency, and compliance. It collects all relevant in-
formation from the LLM and stores it in the Metrics
& Logs Store, which is identified as a data store. This
step is crucial for monitoring the health of the data to
maintain optimal system performance and reliability.
4.2 Security Boundaries
We have identified and defined eight distinct security
boundaries within our DFD, which are described in
Table 2.
4.3 Threat Elicitation
In this section, we conduct a detailed threat elicita-
tion for each component of our system, utilizing the
STRIDE framework in conjunction with the attack
taxonomy outlined in the methods section. Due to
page limitations, we will analyze a single entity, data
flow, process, and data store from the five entities,
thirty-three data flows, seven processes, and four data
stores identified.
Entity. For this analysis, we have chosen the User
entity:
Spoofing: Hijacking User Accounts (Iqbal et al.,
2024) occurs when attackers exploit weak authenti-
cation or stolen credentials to access sensitive pa-
tient data. Hijacking User Machines (Iqbal et al.,
2024) involves using malware or phishing to compro-
mise devices and infiltrate hospital networks. Creden-
tial Stuffing happens when attackers use reused pass-
words from previous breaches to gain unauthorized
access (MITRE, 2024).
Repudiation: Lack of Audit Trails results from in-
adequate logging and weak access controls, allowing
malicious actions to go undetected, such as unautho-
rized alterations of patient records. Manipulation of
Logs occurs when attackers alter or delete log entries
to conceal their activities, making breaches difficult to
trace. User Impersonation exploits weak authentica-
tion and shared accounts to perform actions as another
user, enabling denial of these actions. Unauthorized
Actions on Behalf of Users arise from insufficient au-
thentication and authorization, allowing actions like
unauthorized prescriptions. Insider Threats involve
employees misusing legitimate access to steal data
or perform unauthorized actions, undermining patient
confidentiality and trust.
Data Flow. For this analysis, we have chosen User
to Web Application data flow:
Tampering: Prompt Injection (Jailbreak)
(LLM01) exploits vulnerabilities in LLM-based
systems by accepting unsanitized user inputs due to
inadequate input validation and weak model con-
straints (MITRE, 2024). Attackers can be registered
users with malicious intent or individuals using
compromised accounts who have access to the user
interface and understand the parameter structures,
enabling them to manipulate input fields or API pa-
rameters (Chu et al., 2024). These manipulations can
ICISSP 2025 - 11th International Conference on Information Systems Security and Privacy
330
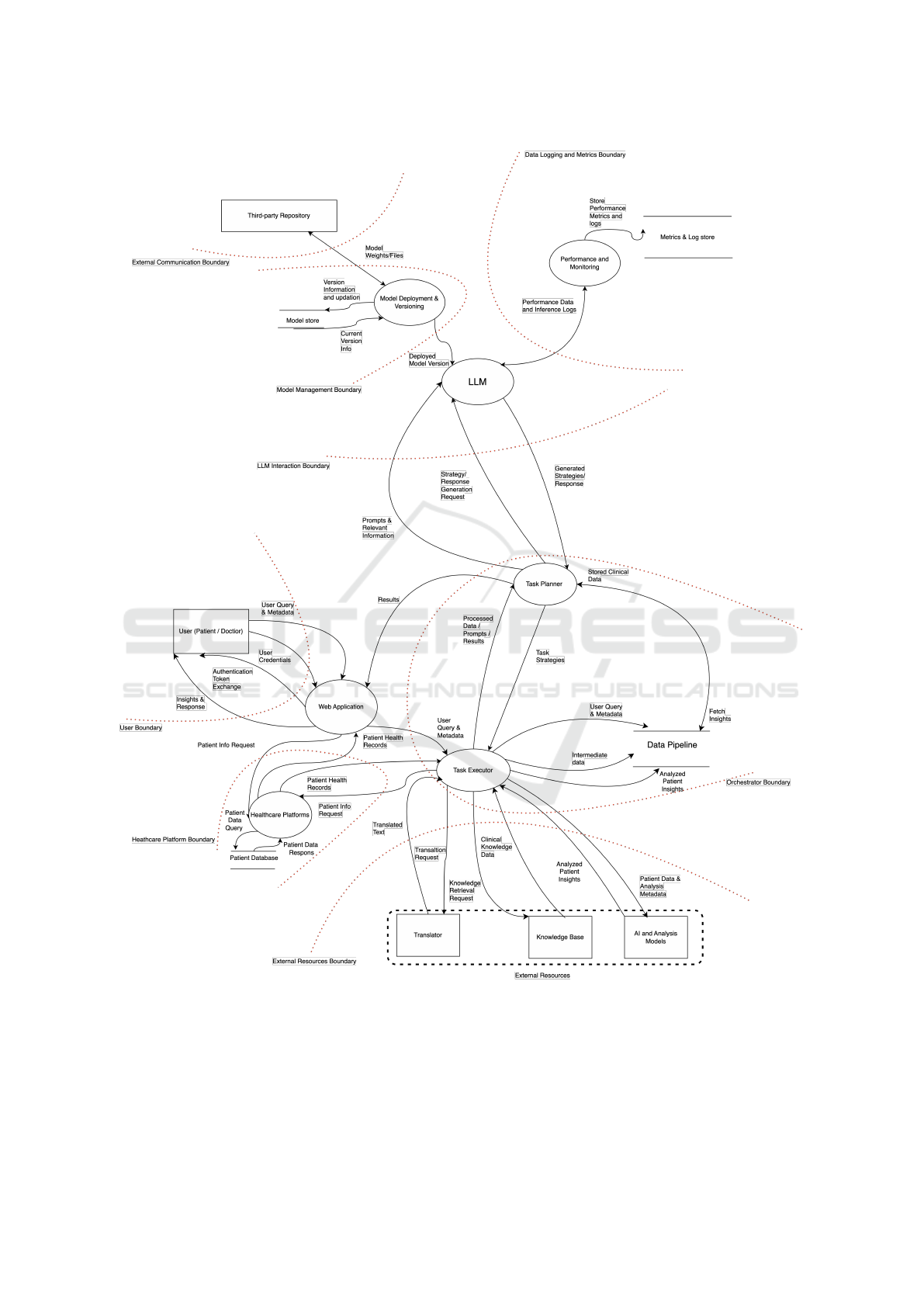
Figure 1: Data Flow Diagram.
lead to unauthorized access to sensitive information,
data breaches, and the generation of misleading or
harmful outputs, thereby compromising the overall
security and integrity of the system.
There are different methods used in this attack
(Chu et al., 2024):Attackers use role-play or style in-
jection to bypass restrictions (Human-Based). Uti-
lizing optimization algorithms to refine prompts and
elicit restricted outputs (Optimization-Based). At-
tackers use encoded or obfuscated prompts to by-
Cyber Threat Modeling of an LLM-Based Healthcare System
331
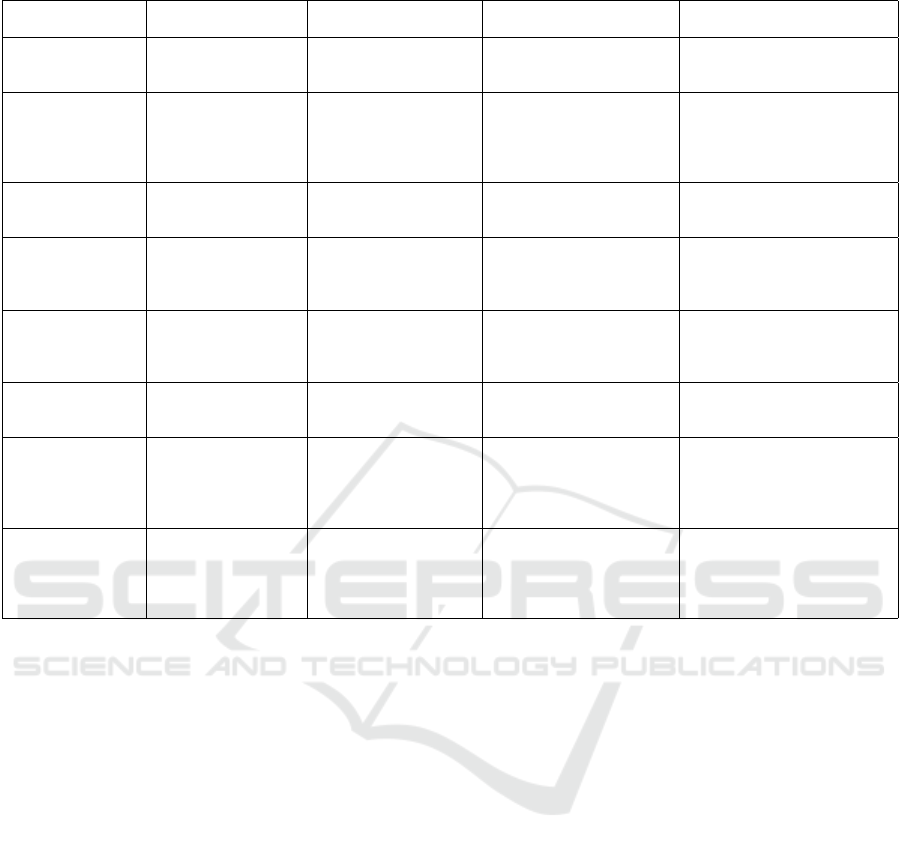
Table 2: Security Boundaries.
Boundary Name Components Inside
Boundary
Trust Assumptions Data Flows Crossing
Boundary
Explanation
User Boundary User (Patient/Doctor) Web Application does
not trust input from ex-
ternal users.
User queries and requests
entering the Web Applica-
tion.
Defines the entry point for ex-
ternal user inputs, which are un-
trusted and need monitoring.
Healthcare Plat-
form Boundary
Healthcare Platform,
Patient Database
Components within this
boundary trust each
other.
Data requests and queries
from Web Application and
Task Executor.
Encompasses components that
store and manage sensitive pa-
tient data, all of which are
trusted internally and secured
with best practices.
External Resources
Boundary
Translator, Knowledge
Base, AI and Analysis
Models
External resources are
untrusted.
Interactions between Or-
chestrator and External
Resources.
Includes third-party tools, fo-
cusing on untrusted data ex-
changes that could be exploited.
Orchestrator
Boundary
Task Executor, Task
Planner, Data Pipeline
Components within this
boundary trust each
other.
Data exchanges with Exter-
nal Resources, Web Appli-
cation, Healthcare Platform,
and LLM.
Groups key orchestrator com-
ponents, emphasizing cautious
handling of untrusted interac-
tions at its edges.
LLM Interaction
Boundary
LLM Data crossing this
boundary cannot be
trusted.
Inputs to and outputs from
the LLM.
Identifies interactions with the
LLM as potential attack sur-
faces due to untrusted data ex-
changes.
External Communi-
cation Boundary
Third-party Reposi-
tory
Third-party Repository
is untrusted.
Interactions between Model
Deployment & Versioning
and Third-party Repository.
Highlights the risk of introduc-
ing malicious code through ex-
ternal model updates.
Model Manage-
ment Boundary
Model Deployment
& Versioning, Model
Store
Components within this
boundary trust each
other.
Data flows from Third-party
Repository or LLM.
Encompasses components man-
aging the LLM, assuming in-
ternal trust while treating exter-
nal data flows as potential attack
surfaces.
Data Logging and
Metrics Boundary
Performance and
Monitoring, Metrics &
Logs Store
Components within this
boundary trust each
other.
Interactions between LLM
and Performance and Mon-
itoring process.
Includes components for log-
ging and monitoring, with data
exchanges across this boundary
considered untrusted and vul-
nerable.
pass content filters (Obfuscation-Based). Modifying
request parameters to alter backend behavior or the
LLM’s output (Parameter-Based). MITM attacks, as
outlined in Table 3, are within this scope, alongside
Replay, HTTP Response Splitting, and XML Injec-
tion attacks.
Information Disclosure: Man-in-the-Middle
(MITM) Attacks can also expose sensitive informa-
tion like patient symptoms and medical histories.
Eavesdropping exploits unencrypted data trans-
missions and insecure communication protocols,
allowing attackers to silently capture sensitive data
such as patient IDs and treatment plans.
Sensitive Information Disclosure (LLM06)
(OWASP, 2024) occurs when LLMs is trained on
sensitive data without adequate safeguards and weak
data privacy controls as LLM memorize sensitive
information from its training data. Attackers can
craft specific queries that exploit this capability and
retrieve confidential data. For example, an attacker
might query, ”Provide an example patient record
similar to ’John Doe’ with epilepsy,” causing the
LLM to disclose sensitive patient details (Rossi et al.,
2024).
Denial of Service: Flooding/DDoS Attack targets
the limited request-handling capacity of web applica-
tion interfaces lacking traffic filtering. In healthcare,
this could involve flooding the interface with numer-
ous simultaneous queries, preventing doctors and pa-
tients from accessing critical medical advice or pa-
tient records.
Data Store. For this analysis, we have chosen the
Data pipeline datastore:
Tampering: Data Manipulation Attacks exploit
weak access controls and insufficient data integrity
checks to alter stored data, such as modifying patient
metadata, which leads to incorrect analyses and com-
promised patient care. Metadata Injection Attacks
take advantage of inadequate input validation to insert
or modify metadata, misleading the system and po-
tentially causing misdiagnoses or inappropriate treat-
ment plans.
Repudiation: Similar to the case of the user entity,
manipulation or deletion of logs and insufficient au-
dit trails allow attackers to erase or alter records, hid-
ing malicious activities like incorrect data insertions
in the Data Pipeline datastore. In healthcare, this can
lead to undetected tampering with patient data, com-
promising data integrity and regulatory compliance.
Information Disclosure: Sensitive Data Exposure
ICISSP 2025 - 11th International Conference on Information Systems Security and Privacy
332

results from inadequate access controls and weak en-
cryption, allowing attackers to access unencrypted pa-
tient data. Unauthorized Data Access arises from
weak access control mechanisms, enabling attackers
with compromised credentials to manipulate or delete
critical health data.
Denial of Service: Flooding/DDoS Attacks on the
Data Pipeline Datastore overload the system with ex-
cessive requests. Unlike attacks on web interfaces,
which disrupt access to services, these target the data
store directly, hindering data retrieval and updates.
Resource Exhaustion via Complex Queries consumes
significant processing power, delaying access to es-
sential healthcare data on time.
Process. For this analysis, we have chosen the LLM
process:
Spoofing: Model version spoofing occurs when an
attacker delivers fake model updates by manipulat-
ing communication channels or versioning requests,
causing the LLM to provide faulty medical advice and
endangering patients. Task Planner spoofing happens
when an attacker impersonates the Task Planner due
to a lack of mutual authentication, enabling them to
send malicious prompts that result in fraudulent re-
sponses and disrupt patient care.
Tampering: Prompt Injection (LLM01) in LLM -
Tampering threats in the LLM process, such as Di-
rect Prompt Injection Jailbreak Attacks, exploit insuf-
ficient input sanitization, allowing attackers to inject
harmful instructions. In healthcare, this could lead
to the LLM issuing unsafe medical advice. Simi-
lar methods outlined in the data flow section for jail-
breaking are applied here as well.
Indirect Prompt Injection occurs when attackers
manipulate external data sources to inject harmful
prompts (Greshake et al., 2023). This is due to the
system’s dependence on external data and the lack
of robust input filtering. Attackers use various meth-
ods (Greshake et al., 2023) such as passive methods,
where malicious prompts are embedded in public data
sources or code repositories. Active methods, where
attackers deliver prompts directly, such as via emails
processed by the systems. User-driven Injections ex-
ploit social engineering, tricking users into copying
and pasting malicious prompts unknowingly. Finally,
Hidden Injections uses obfuscation techniques like
multi-stage exploits or encoded prompts, making de-
tection harder by embedding prompts in images or us-
ing encrypted payloads through executable scripts. In
healthcare, for example, an attacker could manipulate
an external knowledge base response, resulting in in-
accurate medical recommendations from the LLM.
Repudiation: Attackers manipulate LLM logs to
conceal the injection of malicious prompts, prevent-
ing the detection of incorrect patient treatment sug-
gestions. Denial of Query Submission occurs when
inadequate tracking of query history allows attackers
to modify logs and deny responsibility for submitting
malicious queries, resulting in the LLM generating in-
correct medical advice without traceability and pos-
ing significant risks to patient safety.
Information Disclosure: Sensitive Data Exposure
(LLM06) (OWASP, 2024) is a concern here. In
the context of LLMs, attackers can access sensitive
patient data or even training data processed by the
model, leading to breaches of patient confidentiality
and potential misuse of proprietary information. This
can be achieved through methods like prompt injec-
tion, where an attacker crafts inputs to bypass input
filters and convince the LLM to reveal confidential
data that it has memorized or processed.
Insecure Output Handling (LLM02) occurs when
LLM outputs are integrated into external web inter-
faces without proper sanitization (OWASP, 2024). If
an attacker has access to the API or can manipulate
web output, they can inject malicious scripts or code,
such as cross-site scripting (XSS) or cross-site request
forgery (CSRF), through LLM-generated responses
(OWASP, 2024). An attacker injects a script via LLM
output in a patient portal, exploiting XSS to access
sensitive health data.
Denial of Service: Model Denial of Service
(LLM04) occurs when attackers flood the LLM with
a large number of queries, causing it to crash and
preventing doctors from receiving real-time medical
guidance. They also send complex medical queries
that consume significant LLM resources, resulting in
delayed responses for critical patient care. Addition-
ally, overwhelming the LLM with multiple simulta-
neous tasks further delays response times and impacts
timely patient treatment.
Elevation of Privilege: Privilege Escalation
through Model Vulnerabilities occurs when weak ac-
cess controls, such as inadequate RBAC or poorly se-
cured API keys, allow attackers to modify model pa-
rameters or access sensitive data. In a healthcare con-
text, this can enable unauthorized access to patient
data or alteration of treatment algorithms, compro-
mising patient care and privacy.
A selection of attacks is detailed in Table 3, lo-
cated after the References section.
5 DISCUSSION
In this paper, we deployed a third-party LLM (Com-
mercial Off-The-Shelf, or COTS) into our system.
Had we continued to use the LLM as an API, as in the
Cyber Threat Modeling of an LLM-Based Healthcare System
333

referenced system (Abbasian et al., 2024), both sys-
tem modeling and threat evaluation would have been
different. We would have considered the LLM API as
an entity in our DFD, with the primary threats iden-
tified being related to impersonation (Spoofing) and
lack of accountability (Repudiation). The advantages
are that it is easier to set up the system to use LLM
API, and it ensures scalability and that the system is
up to date. However, this also comes with its own
risks, such as DNS spoofing or API Key theft, which
could allow attackers to set up a fake endpoint and
impersonate the LLM API, which could lead to data
manipulation and unauthorized access. Having inad-
equate logging or log manipulation can make verify-
ing actions or detecting malicious activities difficult.
Since we deployed the LLM model into our system,
we can ensure that sensitive information remains in
our secure environment, as there can be vulnerabil-
ities associated with data transmission over external
networks. Ultimately, the decision on how LLM is
adapted into the system is based on the organization’s
priorities and risk tolerance.
Prompt injection attacks are identified in multiple
components of our system - the User-to-Web Applica-
tion data flow and the LLM process. This dual elicita-
tion arises because such attacks exploit the vulnerabil-
ities at different system points. Countermeasures can,
therefore, be implemented at various levels: input fil-
ters can be deployed in the data flow between the user
and the web application to sanitize incoming prompts,
while fine-tuning the LLM can enhance its ability to
reject improper prompts internally. This approach un-
derscores the importance of collaboration between cy-
bersecurity (handling input filtering) and data science
(responsible for model development). These teams
often operate independently, which can hinder the
implementation of comprehensive security measures.
Recognizing and addressing these interdependencies
is crucial during countermeasure analysis, as it allows
for a more effective and cost-efficient defense strategy
against prompt injection attacks.
One of the limitations of our study is that we
did not address the threat of training data poisoning,
as our approach does not involve training or fine-
tuning the models internally. We expect the third-
party providers to maintain security while training
the model through Service Level Agreements (SLAs).
While the threat of training data poisoning is signifi-
cant as it can potentially undermine the reliability and
trustworthiness of the LLM output it remains beyond
the scope of our current work. By acknowledging this
limitation underscores the need for future research to
explore strategies for mitigating such risks.
Additionally, we opted for the STRIDE-per-
element approach instead of STRIDE-per-interaction
in our threat elicitation process (Shostack, 2014).
This decision allows us to more easily associate spe-
cific threats with individual system components, sim-
plifying the process for the technical team and mak-
ing it more accessible to stakeholders who may not
have extensive technical expertise. Using STRIDE-
per-element also supports detailed system modeling.
We can more accurately identify and represent com-
ponents like LLMs, offering a clearer view of poten-
tial vulnerabilities specific to each part of the system.
6 CONCLUSION & FUTURE
WORK
In this paper, we conducted a comprehensive threat
modeling analysis of a healthcare system powered
by large language models (LLMs). By adapting the
STRIDE methodology, we created a system model
and systematic approach to identify component-level
threats and map potential vulnerabilities. In the fu-
ture, we aim to establish tailored countermeasures to
enhance resilience.
7 DECLARATION OF
GENERATIVE AI AND
AI-ASSISTED TECHNOLOGIES
IN THE WRITING PROCESS
During the revision of this work, the author(s) used
ChatGPT (OpenAI’s chat-based AI) for grammar and
language review. The author(s) subsequently re-
viewed and edited the content as needed and take full
responsibility for the publication’s final content.
REFERENCES
Abbasian, M., Azimi, I., Rahmani, A. M., and Jain, R.
(2024). Conversational health agents: A personalized
llm-powered agent framework.
Balloccu, S., Schmidtov
´
a, P., Lango, M., and Du
ˇ
sek, O.
(2024). Leak, cheat, repeat: Data contamination and
evaluation malpractices in closed-source llms.
Brown, H., Lin, L., Kawaguchi, K., and Shieh, M. (2024).
Self-evaluation as a defense against adversarial at-
tacks on llms.
Chen, C. and Shu, K. (2024). Can llm-generated misinfor-
mation be detected?
Chu, J., Liu, Y., Yang, Z., Shen, X., Backes, M., and Zhang,
Y. (2024). Comprehensive assessment of jailbreak at-
tacks against llms.
ICISSP 2025 - 11th International Conference on Information Systems Security and Privacy
334

Deng, G., Liu, Y., Li, Y., Wang, K., Zhang, Y., Li, Z., Wang,
H., Zhang, T., and Liu, Y. (2024). Masterkey: Auto-
mated jailbreaking of large language model chatbots.
In Proceedings 2024 Network and Distributed System
Security Symposium. Internet Society.
Deng, M., Wuyts, K., Scandariato, R., Preneel, B., and
Joosen, W. (2011). A privacy threat analysis frame-
work: supporting the elicitation and fulfillment of
privacy requirements. Requirements Engineering,
16(1):3–32.
Finlayson, M., Ren, X., and Swayamdipta, S. (2024). Logits
of api-protected llms leak proprietary information.
Greshake, K., Abdelnabi, S., Mishra, S., Endres, C., Holz,
T., and Fritz, M. (2023). Not what you’ve signed up
for: Compromising real-world llm-integrated applica-
tions with indirect prompt injection.
I. S. Authority (2024). Tehisintellekti ja Masin
˜
oppe
Tehnoloogia Riskide ja Nende Leevendamise
V
˜
oimaluste Uuring.
IBM (2024). What Are Large Language Model Operations
(LLMOps)? Accessed: 2024-11-13.
Iqbal, U., Kohno, T., and Roesner, F. (2024). Llm platform
security: Applying a systematic evaluation framework
to openai’s chatgpt plugins.
MITRE (2024). Atlas matrix. Accessed: Oct 21, 2024.
OWASP (2024). Owasp top 10 for large language model
applications. Accessed: Oct 21, 2024.
Pankajakshan, R., Biswal, S., Govindarajulu, Y., and Gres-
sel, G. (2024). Mapping llm security landscapes: A
comprehensive stakeholder risk assessment proposal.
Papernot, N., McDaniel, P., Sinha, A., and Wellman, M. P.
(2018). SoK: Security and Privacy in Machine Learn-
ing. In 2018 IEEE European Symposium on Security
and Privacy (EuroS&P), pages 399–414. IEEE.
Pathmanathan, P., Chakraborty, S., Liu, X., Liang, Y., and
Huang, F. (2024). Is poisoning a real threat to llm
alignment? maybe more so than you think.
Rossi, S., Michel, A. M., Mukkamala, R. R., and Thatcher,
J. B. (2024). An early categorization of prompt injec-
tion attacks on large language models.
Shah, S. B., Thapa, S., Acharya, A., Rauniyar, K., Poudel,
S., Jain, S., Masood, A., and Naseem, U. (2024). Nav-
igating the web of disinformation and misinforma-
tion: Large language models as double-edged swords.
IEEE Access.
Shi, C., Liang, P., Wu, Y., Zhan, T., and Jin, Z. (2024). Max-
imizing User Experience with LLMOps-Driven Per-
sonalized Recommendation Systems.
Shostack, A. (2014). Threat Modeling: Designing for Se-
curity. John Wiley & Sons.
Tang, X., Jin, Q., Zhu, K., Yuan, T., Zhang, Y., Zhou, W.,
Qu, M., Zhao, Y., Tang, J., Zhang, Z., Cohan, A., Lu,
Z., and Gerstein, M. (2024). Prioritizing safeguarding
over autonomy: Risks of llm agents for science.
Tete, S. B. (2024). Threat modelling and risk analysis for
large language model (llm)-powered applications.
Truong, J. B., Maini, P., Walls, R. J., and Papernot, N.
(2021). Data-free model extraction.
Vassilev, A., Oprea, A., Fordyce, A., and Anderson, H.
(2023). NIST Trustworthy and Responsible AI NIST AI
100-2e2023 Adversarial Machine Learning: A Tax-
onomy and Terminology of Attacks and Mitigations.
NIST. Available at https://doi.org/10.6028/NIST.AI.
100-2e2023, Accessed Oct 21, 2024.
Zhao, W., Khazanchi, V., Xing, H., He, X., Xu, Q., and
Lane, N. D. (2024). Attacks on third-party apis of
large language models.
Cyber Threat Modeling of an LLM-Based Healthcare System
335
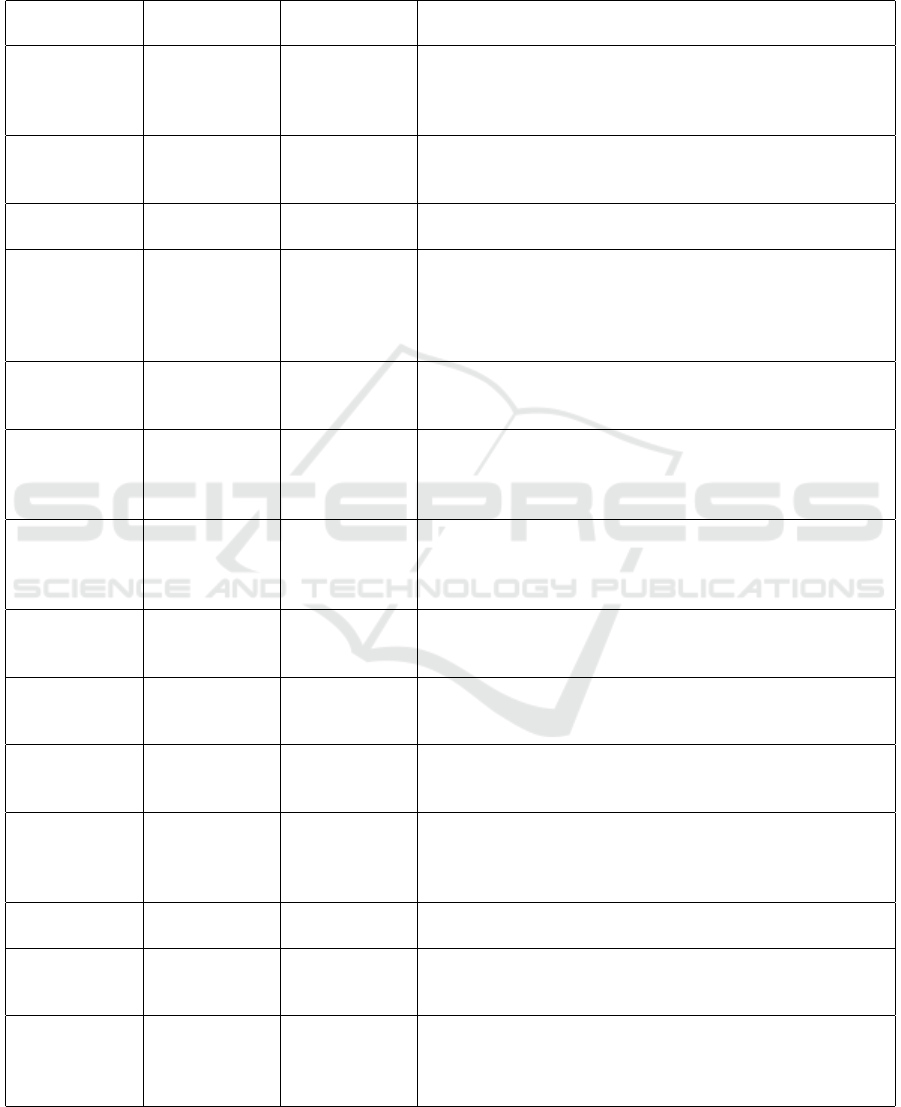
APPENDIX
Table 3: Threat Elicitation Table (selected samples). Type - Conventional Cyber Threats: CCT, Adversarial Threats: AdvT,
Conversational Threats: ConT DFD Elements - E: Entity, DF: Data Flow, P: Process, DS: Data Store.
Type DFD Element Identified
Threats
Threat Description
AdvT User to Web
Application
(DF), LLM
(P)
Sensitive
Information
Disclosure
(LLM06)
Exploitation of LLM memory to retrieve confidential data
by crafting specific queries (OWASP, 2024) (MITRE,
2024).
AdvT LLM (P) Model Denial
of Service
(LLM04)
An attacker overloads resource usage or manipulates the
context window to degrade LLM performance and increase
operational costs (OWASP, 2024) (MITRE, 2024).
AdvT LLM (P) Model Ver-
sion Spoofing
Attackers deliver fake model updates, causing compro-
mised model behavior and inaccurate healthcare advice.
AdvT LLM (P) Privilege
Escalation
through
Model Vul-
nerabilities
Weak access control and poor API security allow attackers
to access and alter sensitive model parameters.
AdvT LLM (P) Insecure Out-
put Handling
(LLM02)
Poor sanitization of LLM outputs allows attackers to inject
malicious scripts, risking unauthorized access to sensitive
data
ConT User to Web
Application
(DF), LLM
(P)
Prompt
Injection (Jail-
break)
Attackers exploit input validation weaknesses to manipu-
late prompts, potentially generating unsafe medical advice
(OWASP, 2024)
ConT LLM (P) Resource
Exhaustion
via Prompt
Manipulation
Attackers overwhelm the system by crafting computation-
ally intensive prompts, causing service degradation.
ConT LLM (P) Indirect
Prompt Injec-
tion
Manipulation of external sources allows attackers to in-
ject harmful prompts, generating inaccurate responses
(OWASP, 2024) (MITRE, 2024).
CCT User (E) Browser Ses-
sion Hijacking
Exploiting weak session management, attackers intercept
session tokens to impersonate users and access sensitive
data.
CCT User (E), Data
Pipeline (DS),
LLM (P)
Manipulation
of Logs
Attackers alter or delete log files to conceal malicious ac-
tivities and evade detection.
CCT User to Web
Application
(DF)
Man-in-
the-Middle
(MITM) At-
tack
Attackers intercept and alter unencrypted communication,
exposing sensitive data and potentially misguiding treat-
ment.
CCT Data Pipeline
(DS)
Data Manipu-
lation Attack
Attackers alter stored data due to weak access controls, im-
pacting data integrity and healthcare decisions.
CCT Data Pipeline
(DS), LLM
(P)
Sensitive Data
Exposure
Inadequate encryption and access control lead to unautho-
rized access to sensitive patient data.
CCT User to Web
Application
(DF)
Exploiting
Vulnerabili-
ties for Denial
of Service
Attackers exploit unpatched vulnerabilities in the web ap-
plication, causing system crashes and unavailability of
healthcare resources.
ICISSP 2025 - 11th International Conference on Information Systems Security and Privacy
336
