
Digital Medication Prescription System with JSON
Liverson Paulo Furtado Severo
a
and Jean Everson Martina
b
Department of Informatics and Statistics, Federal University of Santa Catarina, Florian
´
opolis, Santa Catarina, Brazil
Keywords:
JSON, JWS, FHIR, JAdES, Signature, Interoperability.
Abstract:
The rapid evolution of digital health solutions, accelerated by the COVID-19 pandemic, highlighted the ne-
cessity for secure and efficient electronic prescription and medication dispensing systems. This paper presents
a study on integrating HL7 FHIR standards and JAdES signatures to facilitate the digitalization of healthcare
documentation. By addressing key challenges such as interoperability, data volatility, and security, the research
proposes a framework that ensures the authenticity and integrity of electronic prescriptions—Emphasizing the
importance of self-contained digital documents that eliminate reliance on external references to enhance the
reliability of health information exchange in Brazil. Furthermore, it outlines the legal implications of elec-
tronic signatures in Brazil, advocating for compliance with national standards to ensure the legal validity of
digital prescriptions. The findings indicate that the proposed solutions not only streamline healthcare processes
but also foster a gradual transition from traditional paper-based systems to a robust digital infrastructure, ulti-
mately improving patient care and operational efficiency in the healthcare sector.
1 INTRODUCTION
Like the rest of the world, Brazil faced a significant
health crisis due to the COVID-19 pandemic. This
situation accelerated the adoption of electronic medi-
cal documents and their digital processing (Conselho
Federal de Medicina, 2021). Brazilian law states
these documents can be electronically signed with
legal validity. However, qualified electronic signa-
tures are mandatory for special control prescriptions
and medical certificates (Presid
ˆ
encia da Rep
´
ublica do
Brasil, 2020).
Currently, in Brazil, prescriptions and medication
dispensing are issued through printed documents with
a handwritten signature, and dispensing is done all at
once. This system is inflexible to the patient and has
security issues related to falsification, problems with
prescription legibility, and lack of traceability.
The aim is to transform this process by using digi-
tal technologies and introducing a new concept of par-
tial dispensing, where patients can access medications
gradually based on their needs. Electronic signatures
represent a crucial step in facilitating the flow of dig-
ital documents, making it easier to share information,
streamline bureaucratic processes, and enhance stor-
age solutions.
a
https://orcid.org/0009-0006-3962-8593
b
https://orcid.org/0000-0003-4104-1741
Electronic signatures are a way to authenticate and
validate documents digitally using tools specifically
developed for this purpose. There are three categories
of electronic signatures. The simple electronic signa-
ture is similar to traditional signatures made on pa-
per. The advanced electronic signature employs cryp-
tographic algorithms to ensure the signature cannot
be forged. Finally, the qualified electronic signature
is used in more specific contexts, incorporating time-
stamping and offering greater robustness. These cat-
egories serve different needs and levels of security in
the digital signing process.
Electronic signatures can be categorized as em-
bedded or detached. Embedded signatures are inte-
grated with the document, resulting in a single signed
document. In contrast, detached signatures sepa-
rate the document and the signature into two files.
These two components demonstrate that the signature
is valid when submitted for validation.
Qualified signatures are advanced signatures cre-
ated using a qualified signature creation device based
on certification qualifications for electronic signa-
tures (European Parliament and Council of the Eu-
ropean Union, 2014). In Brazil, a qualified signa-
ture complies with the terms outlined in Law No.
14,063 regarding qualified signatures (Presid
ˆ
encia da
Rep
´
ublica do Brasil, 2020).
834
Severo, L. P. F. and Martina, J. E.
Digital Medication Prescription System with JSON.
DOI: 10.5220/0013315700003911
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 18th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2025) - Volume 2: HEALTHINF, pages 834-843
ISBN: 978-989-758-731-3; ISSN: 2184-4305
Proceedings Copyright © 2025 by SCITEPRESS – Science and Technology Publications, Lda.

This framework has paved the way for the evolu-
tion of signatures in the health sector; however, there
are still potential improvements to be addressed. One
area that requires enhancement is the interoperabil-
ity of signed patient documents, as there is currently
no standardization to facilitate information exchange
between different healthcare institutions. To address
the issue of data interoperability, the National Health
Data Network (RNDS) project was initiated, aimed
at the digital transformation of healthcare in Brazil
(Minist
´
erio da Sa
´
ude do Brasil, 2020). Interoperabil-
ity can be understood as the standardization of vocab-
ularies, data representation structures, and messaging
protocols between systems. However, the develop-
ment of these standards is slow, and their adoption is
even slower (Roehrs et al., 2021).
The RNDS project uses the Fast Healthcare Inter-
operability Resources (FHIR) standard Health Level
Seven International (HL7) created for data files to en-
hance interoperability. To enable the use of files gen-
erated in the FHIR standard, they must be transformed
into digital documents, as relevant information must
be self-contained for them to qualify as such. In the
case of HL7 FHIR, external references for pertinent
details may pertain to the healthcare provider or the
patient.
Despite this, using the FHIR standard can facili-
tate the electronic registration and dispensing of med-
ical prescriptions. A medical prescription document
must be signed by a physician in a manner that al-
lows for determining when the signature was made
and ensures that the physician has the authorization to
practice, as stipulated by the Federal Medical Coun-
cil (CFM) and registered with the Regional Medi-
cal Council (CRM) of the physician (Presid
ˆ
encia da
Rep
´
ublica do Brasil, 1957).
To dispense medications, it is essential to ensure
that the pharmacist is authorized to practice, as indi-
cated by their registration with the Federal Pharmacy
Council (CFF) (Presid
ˆ
encia da Rep
´
ublica do Brasil,
1960). Therefore, during the dispensing process, a
separate file is created solely for the total or partial
dispensing of the prescribed medications. This file
must also be signed, including information on when
the signature was made.
The hypothesis is that the HL7 FHIR pattern with
digital signature JAdES effectively enhances the in-
teroperability and the security of the prescription and
dispensation of medicines in Brazil, promoting a pro-
cess transition from paper to robust digital infrastruc-
ture. To do that, this research looks to develop a dig-
ital system to prescribe and dispense medicines, ex-
ploring technologies such as the pattern HL7 FHIR
and JAdES digital signatures. The following features:
• Allow the generation of digital prescript and its
registration with support to the partial dispensa-
tion of medicines;
• Validation of documents through APIs and the im-
plementation of a database to control the dispen-
sation of medicines;
• Implement an interoperability and signature pat-
tern to medical prescriptions and dispensations;
• Validation of the project in a controlled environ-
ment.
2 SIGNATURE IN DOCUMENTS
IN JSON FORMAT
Despite the existence of other formats, such as XML,
JSON is a simple format that provides the necessary
structures for information exchange and can be self-
explanatory for humans (Pohls, 2015). JSON syntax
has increasingly become prevalent in electronic trans-
actions, extending beyond just support for web tokens
(JWT). As a result, the JSON Web Signature (JWS)
has been defined for digital signatures (Ibarz, 2020).
2.1 JWS
According to (Jones et al., 2015), JWS represents se-
cure content using signatures or message authenti-
cation codes (MACs) with data structures based on
JSON and Base64 encoding. Three fields are used in
the composition of these structures: the JSON Object
Signing and Encryption (JOSE) header, the JWS pay-
load, and the JWS signature.
The JOSE header is a JSON object that contains a
description of cryptographic operations and parame-
ters used, all compressed into header parameters. It
consists of a protected JWS header and an unpro-
tected JWS header, where the protected header in-
cludes parameters whose integrity is ensured by the
JWS signature. In contrast, the unprotected header
lacks this integrity protection. The JWS payload is the
message that must be secured in octet format, which
can be in an arbitrary sequence. The JWS signature
is the digital signature or MAC that protects both the
protected JWS header and the JWS payload.
JWS can be serialized in two forms: JWS Com-
pact Serialization and JWS JSON Serialization. In
JWS Compact Serialization, the unprotected header
is not used; thus, the JOSE header and the pro-
tected JWS header are the same. The JOSE header,
JWS payload, and JWS signature are concatenated
as Base64-encoded strings, separated by periods. In
contrast, JWS JSON Serialization requires at least
Digital Medication Prescription System with JSON
835

one of the headers mentioned above, or both, with
the JOSE header representing the combination of the
header information (Jones et al., 2015). Figure 1 il-
lustrates an example of a JWS signature.
Figure 1: JWS signature example.
2.2 JAdES Signature
In 1999, the European Telecommunications Stan-
dards Institute (ETSI) established the ETSI Elec-
tronic Signatures and Infrastructures Working Group,
a committee focused on developing the European
standard for digital signatures and related infrastruc-
tures (Ibarz, 2020). According to (Kutyłowski and
Bła
´
skiewicz, 2023), these signatures possess the fol-
lowing characteristics:
• They are uniquely linked to a signer;
• They are capable of identifying the signer;
• They are created using electronic signature cre-
ation data that the signer can use exclusively and
with a high level of confidentiality;
• They are connected to the signed data so that any
subsequent changes will be detected.
After updates, the committee published the Euro-
pean standards, approved by the National Standard-
ization Organizations of the European Union Member
States, which defined the family of Advanced Elec-
tronic Signatures (AdES) for digital signatures. The
following features characterize these:
• A set of signed and unsigned attributes with a spe-
cific syntax (initially using ASN.1 dictionaries,
followed by XML, PDF, and later JSON);
• Mechanisms to incorporate these attributes into
the digital signature structure;
• A series of signed and unsigned attributes combi-
nations are called levels.
In the case of basic electronic signatures, if the
signing certificate expires, the signature automatically
becomes invalid. To address this issue, formats al-
low incorporating additional information in the sig-
nature to ensure long-term validity. This information
includes evidence from a third party (such as certifi-
cation authorities) and time stamps in the signature to
verify the status of the signature at the moment it was
created (Ibarz, 2021).
In 2021, a new advanced electronic signature was
created using JWS, known as JAdES. The general
requirements for a JAdES signature are the compo-
nents defined in the JOSE header (Ibarz, 2020). For
a JAdES signature to be valid, it must not only con-
tain the header parameters of a JWS but also include
new parameters for signature qualification based on
the specified level. JAdES features four classification
levels that function incrementally, each designed to be
used according to the application’s needs. The avail-
able levels are:
• Level B-B incorporates signed header parameters
and some unsigned components within the un-
signed header parameter etsiU when the signature
is generated.
• Level B-T requires the generation and inclusion
of a trust token that proves the signature existed at
a specific date and time in an existing signature.
• Level B-LT mandates incorporating all signature
validation materials into the signature document,
allowing for the long-term availability of valida-
tion materials.
• Level B-LTA necessitates the inclusion of time
stamps that enable the validation of the signature
for extended periods after its creation, ensuring
the long-term validation and integrity of the doc-
ument.
The first level is the simplest to implement, re-
quiring fewer parameters to create. Generally, this
advanced signature utilizes the header parameters al-
ready defined as mandatory by the JWS signature,
adds the requirement for optional JWS parameters,
and introduces new parameters.
HEALTHINF 2025 - 18th International Conference on Health Informatics
836
The header parameter JWS defines as mandatory
for a signature is the Algorithm (alg). This parameter
is protected and serves to identify the cryptographic
algorithm used for the security of the JWS. There-
fore, a JWS signature will be invalid if the alg does
not contain a supported algorithm or if no associated
cryptographic algorithm exists for the MAC content
(Jones et al., 2015). The mandatory header parameter
defined for a JAdES signature is the Claiming Sign-
ing Time (sigT). This is a protected parameter whose
function is to specify the moment the signer intends
to perform the signing process. Thus, the record must
include a string in Coordinated Universal Time (UTC)
format indicating the time of the signature.
The protected header parameter Critical indicates
which extension parameters are used in the signature
and must be processed and understood. Thus, a list
that should never be empty is generated when it in-
cludes parameters that need to be processed (Jones
et al., 2015). In the case of JAdES, the attributes eligi-
ble to be included in the Critical list are: sigT, x5t#o,
sigX5ts, srCms, sigPl, srAts, adoTst and sigPId (In-
stitute, 2021). The content type (cty) header param-
eter is used to indicate the media type contained in
the JWS payload of the document. This parameter is
included when more than one type of object may be
present in the JWS payload, allowing the application
to use the value of this parameter to eliminate ambi-
guity regarding the data that may be present in the
document.
The header parameters X.509 Certificate SHA-
256 Thumbprint (x5t#S256), X.509 Certificate Digest
(x5t#o), and X.509 Certificates Digests (sigX5ts) are
protected parameters intended to indicate the message
digest responsible for hashing the document. The
x5t#S256 was defined in JWS as an optional attribute
and is specific for use with SHA-256. The parameters
x5t#o and sigX5ts are defined by JAdES, where x5t#o
is used for any hashing algorithm other than SHA-
256, while sigX5ts is utilized when multiple certifi-
cates are used in the signature. In addition to defin-
ing the requirements for the parameters as mentioned
above, the deprecation of the X.509 Certificate SHA-
1 (x5t) defined for JWS signatures is noted due to
its vulnerability, making it easier to break encryption
and retrieve information from the signature (Institute,
2021).
The header parameter X.509 Certificate Chain
(x5c) contains the X.509 public key certificate or the
chain of certificates corresponding to the key used to
sign the JWS digitally. Thus, x5c is a list of cer-
tificates represented as a string value in Base64 for-
mat. This parameter must be present if the parameters
x5t#S256, x5t#o or sigX5ts are not included; other-
wise, its inclusion is optional. In addition to includ-
ing protected parameters, it is possible to add unpro-
tected parameters, which are inserted into a list of pa-
rameters called etsi Unsigned (etsiU), with all entries
formatted in Base64. Table 1 shows the minimum pa-
rameters required for creating a JAdES document at
level B-B.
Table 1: Minimun parameters needed to create a JAdES sig-
nature.
Parameter Mandatory level
Alg Mandatory
SigT Mandatory
Crit Mandatory (sigT)
Cty Mandatory (multiple media)
X5t#S256 Conditioned (without x5c, x5t#o, sigX5ts)
X5t#o Conditioned (without x5c, x5t#S256, sigX5ts)
SigX5ts Conditioned (without x5c, x5t#o, x5t#S256)
X5c Conditioned (without x5t#S256, x5t#o, sigX5ts)
3 HL7 FHIR
HL7 is a nonprofit organization providing frame-
works and standards that facilitate the exchange, in-
tegration, sharing, and retrieval of electronic health
information to support clinical practices and the han-
dling, delivery, and verification of healthcare services
(Health Level Seven International, 2023). HL7 FHIR
is a platform specification that defines a set of capabil-
ities for interoperability processes within the health-
care sector (Health Level Seven International, 2023).
According to (Monsen et al., 2023), it is a solution for
sharing health data information using modular com-
ponents, with numerous developers working tirelessly
to contribute to various specification components that
can be utilized in different contexts, such as best prac-
tice guidelines, clinical document architecture trans-
lation, and clinical care of injuries.
Before the HL7 FHIR standard, other standards
were developed with the same purpose. Still, they had
a lower level of human-readable abstraction, which
resulted in greater effort required for data interpre-
tation. One example is HL7 V2, created in 1989 to
integrate various hospital systems, including admin-
istrative processes and clinical systems (Bender and
Sartipi, 2013). Despite its application, the HL7 V2
standard lacked good scalability. It could not adapt to
other use cases, such as the judicial system, and was
difficult to comprehend, as illustrated in Algorithm 1.
The next standard developed was HL7 V3, created
in 1995 to address the deficiencies of its predecessor.
Semantic and lexical element structures were defined
for this standard to generate message artifacts auto-
matically. However, the standards are not directly im-
plementable and require tools to create software sys-
tems. It offers available XML schemas but not norma-
Digital Medication Prescription System with JSON
837

1 MSH | ˆ˜\& | R e gion a l MP I || Ma s ter MPI | A lph a
Hosp i tal |2006 0 5 01
2 14 0 010|| ADT ˆ A28 | 3 94837 5 | PˆT | 2 .4||| ER <cr
>
3 EV N | A 28 | 2 0 0 6 0 5 0 1 1 4 0 0 0 8 | | | 0 0 0 3 3 8 4 7 5 ˆ
Aut h or ˆ Art h ur ˆ ˆ ˆˆˆ
4 ˆ R egion a l MPI
&2.16.840.1.113883.19 . 2 0 1 & I SO ˆ L
|200 6 05011 4 0008 < cr >
5 PI D | ||000197 2 4 5 ˆ ˆ ˆ N a t ionalP N
&2.16.840.1.1138 8 3 . 1 9 . 3 & I SO ˆ PN
˜45 3 2ˆˆ
6 ˆ C a r e f u lCareClini c
&2.16.840.1.113883.19.2.400566& I SO ˆ
PI ˜ 32423 4 6 ˆ ˆ
7 ˆ G oodma n G P
&2.16.840.1.113883.19.2.450998& I SO ˆ
PI ||
8 Patie n t ˆ P artic i a ˆˆˆˆ ˆ L | | 1 975010 3 | F ||
9 | R a ndomr o a d 23 a& R andom r o a d &23 a ˆˆ
Any t own ˆˆ12 0 0ˆˆ H ||
10 55 5 354 2 557ˆ ORN ˆ PH ˜55 5 354 2 5 58ˆ ORN ˆ FX
|555 555 7 865ˆ WPN ˆ PH < cr >
11 PV 1 || N | < cr >
Algorithm 1: Example of a HL7 V2 message.
tive ones, primarily for verification purposes. Despite
the evolution of the model, the use of HL7 V3 in-
volves complex transformations of models, operating
at a level similar to that of a compiler.
HL7 FHIR was created in 2011, building on
the standards that preceded it and combining their
advantages with modern data transfer technologies.
The standard specification provides basic resources,
frameworks, APIs, and a platform for implement-
ing different solutions. To address information not
included in the basic resources, HL7 FHIR of-
fers an embedded extension mechanism that can be
adapted for specific use cases to ensure interoper-
ability. Therefore, this standard can cover different
healthcare domains and manage resources, making
it suitable for various purposes, contexts, and work-
flows (Vorisek et al., 2022).
There are two main types of FHIR solutions: re-
sources and profiles (Monsen et al., 2023). Resources
are data organized in packages that can be formatted
in JSON or Extensible Markup Language (XML) and
transported using HTTPS. Profiles are the rules for
data exchange, including constraints and additional
data elements (Duda et al., 2022). Implementation
guides serve as procedural standards for the consistent
use of FHIR resources and support Application Pro-
gramming Interfaces (APIs) to facilitate workflows in
specific domains (Duda et al., 2022). FHIR resources
have the following characteristics (Bender and Sar-
tipi, 2013):
• They must have a clear boundary that corresponds
to one or more logical transaction scopes;
• They must be different in meaning, not just in us-
age;
• They need to have a natural identity;
• They should be very common and widely used in
commercial transactions;
• They must not be too specific or detailed to hinder
support for a wide range of commercial transac-
tions;
• They must be mutually exclusive;
• They can use other resources but must not be
merely a composition of resources;
• They need to provide new content;
• They should be recognized within a logical frame-
work based on the similarity of the resource and
what it is connected to;
• They must be large enough to have a meaningful
context.
4 CORRELATED WORKS
The exploration of FHIR resources for interoperabil-
ity is not a new concept. In the research by (Monsen
et al., 2023), the technology is employed to standard-
ize nursing practices to improve the quality of data
outputs. This information can be utilized within the
standard for assessments, care planning, and outcome
measurement, demonstrating its potential to enhance
data transmission, information storage, and knowl-
edge discovery in nursing and public health. Their
research shows the utility of FHIR in creating stan-
dardized healthcare data focused on the nursing sec-
tor and does not address the digital signature require-
ments critical for secure prescription and medication
dispensing processes. While this study focuses on us-
ing the standard for nursing data interoperability, it
does not explore the use of digital signatures to ensure
the authenticity of documents, a crucial factor for the
functionality of prescription and medication dispens-
ing addressed in this article’s study.
The study by (Bender and Sartipi, 2013) compares
the evolutions of the standards set by HL7, highlight-
ing the properties of each standard that allow for a
comparison of their strengths and weaknesses. It em-
phasizes that the FHIR standard has garnered signif-
icant attention from the relevant community due to
its simplicity and the potential for FHIR to leverage
the experiences gained from the implementations of
HEALTHINF 2025 - 18th International Conference on Health Informatics
838

preceding standards to enhance the state of commu-
nication in healthcare systems. Therefore, their study
highlights FHIR’s potential for improving healthcare
communication but lacks the possibility of using a file
with an FHIR pattern as an authenticated digital doc-
ument and digital signatures to use these documents
to prescribe medications and create a rastreability on
it.
(Vorisek et al., 2022) analyzes the benefits of HL7
FHIR in improving the interoperability of health in-
formation. This article compiles a review of existing
literature to enhance understanding of the standard,
with less emphasis on its application. Thus, the arti-
cle aims to identify potential use cases for HL7 FHIR
in health research while highlighting the associated
limitations and providing a realistic perspective on its
implementation in medical research. While the article
identifies potential use cases for HL7 FHIR in health
research, it does not address practical applications in-
volving digital signatures to ensure the authenticity
and security of medical documents, a gap this study
aims to fill.
(Gruendner et al., 2021) developed a preprocess-
ing service to enable the direct loading of FHIR data.
The data is transformed into ready-to-analyze subsets,
converting JSON information into PostgreSQL data
format. This facilitates the transition from data acqui-
sition to relevant clinical research, allowing for more
efficient handling of large-scale clinical data without
reliance on cloud servers. While the study focuses
on storing data without needing cloud servers, it does
not address the resolution of data exchange between
healthcare centers and pharmacies. Consequently, it
does not bring the need for data validation within the
database, as demonstrated in the project presented in
this article.
(Cheng et al., 2021) introduces a module for clini-
cal data interoperability services to the REDCap soft-
ware, designed to create databases for clinical trial re-
search and any electronic health record systems that
utilize the HL7 FHIR standard. This module facili-
tates the independent collection and mapping of data
to REDCap fields while enabling real-time data ex-
traction to support data collection for clinical studies
through intuitive interfaces requiring minimal IT in-
volvement. Although the survey implements FHIR
interoperability to facilitate the collection and map-
ping of clinical data, it does not address the use of dig-
ital signatures to authenticate documents, a key fea-
ture explored in the present work to ensure security
and compliance in medical prescriptions.
(Georgioska, 2020) aimed to analyze the practical
feasibility of using digital signatures in the public pro-
curement system of North Macedonia. The objective
was to enhance the security and authenticity of docu-
ments, primarily focusing on providing a method for
verifying the signer’s identity to ensure the authen-
ticity of signed data. The research demonstrates sig-
nificant effectiveness in security and improves pro-
curement processes’ efficiency by reducing bureau-
cratic paperwork and fostering better communication
among the parties involved. Although the study ex-
plores the use of digital signatures to ensure secu-
rity and authenticity in public procurement systems,
it does not address the application of these technolo-
gies in the healthcare sector, particularly in the con-
text of digital prescriptions and medication dispens-
ing, which is the focus of this study.
5 METHODOLOGY
To digitalize prescription and medication dispensing
documents, it was essential first to understand the
standards used for information exchange in health-
care. In the medical field, HL7 is renowned for its
data standardization, having established HL7 V2 and
HL7 V3 as initial solutions for health information
standardization. However, despite well-established
standards, interpreting data within these frameworks
requires significant effort, and developing an applica-
tion capable of performing this interpretation poses an
even greater challenge.
Thus, the search shifted toward the evolving HL7
FHIR standard, which has shown great potential. This
standard employs more user-friendly formats that fa-
cilitate easier association and transport, reducing ef-
fort for humans and applications in data interpreta-
tion. Among the possible formats for generating a file
in HL7 FHIR are JSON and XML, which are more
manageable for applications and can effectively sup-
port electronic document signatures.
With its high capacity for information transfer and
low storage and memory requirements, along with the
ease of understanding the contained information due
to the hierarchical organization within the file, the
JSON format has proven to be the ideal choice for
advancing the next steps of the research. In contrast,
while XML also has a well-defined hierarchical struc-
ture, it requires more effort for data transition and in-
terpretation, as illustrated in Table 2.
There were issues to be resolved regarding using
HL7 FHIR, particularly due to the reliance on hy-
perlinks as references. While bundles and contained
resources are used, references with links associated
with those bundles remain possible. This approach
hindered the creation of a signed document, as a dig-
itally signed document must contain its entire scope.
Digital Medication Prescription System with JSON
839
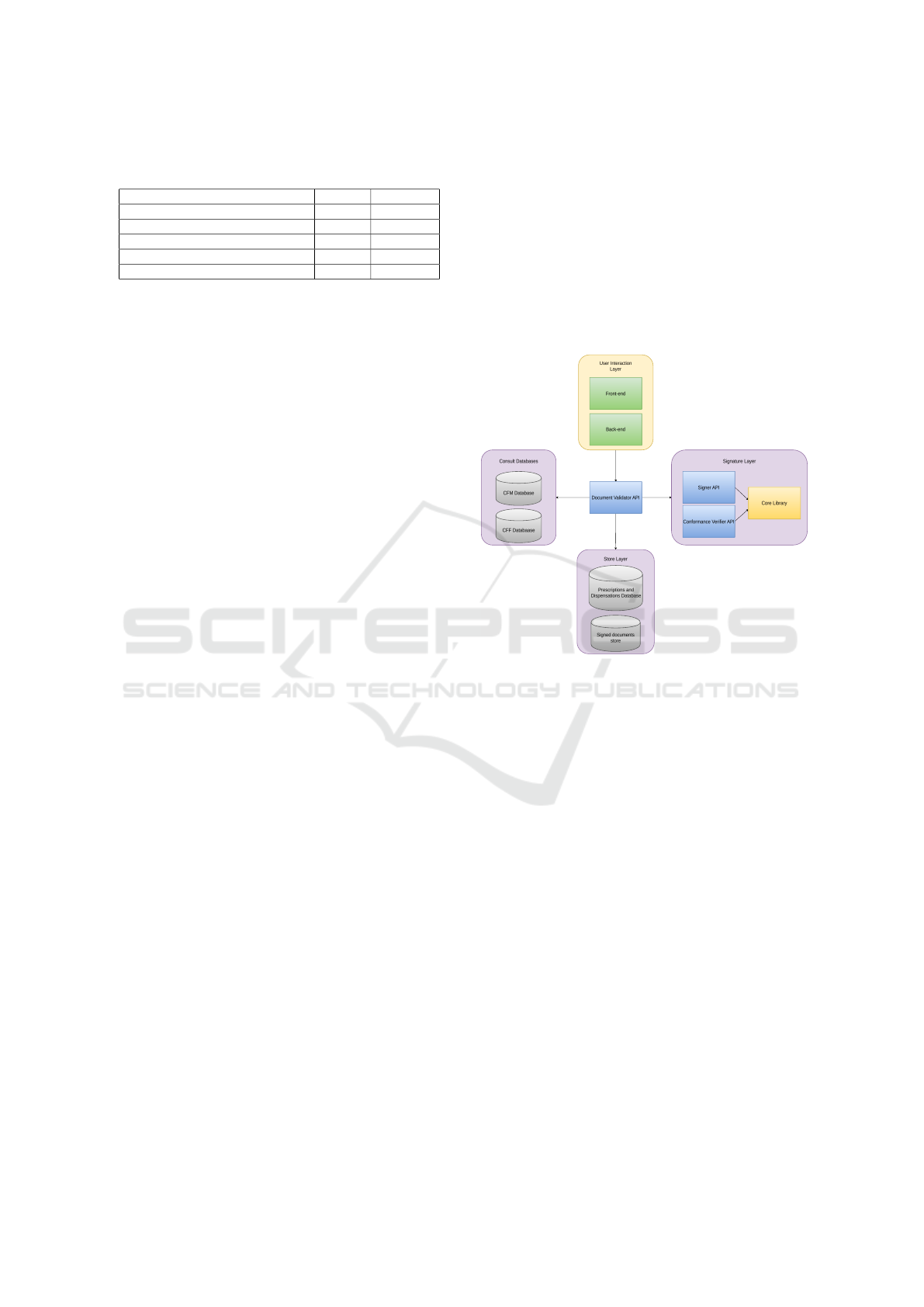
Table 2: Comparison between JSON and XML adapted
from (Nurseitov et al., 2009).
JSON XML
Number Of Objects 100000 100000
Total Time(ms) 7497.36 310017.47
Average Time(ms) 0.07 3.10
Average System % CPU Utilization 11.30 36
Average memory % utilization 68.06 68.79
Furthermore, these references are volatile and would
invalidate the generated prescription because of the
information change after the signature. To address
this, these references were incorporated into the doc-
ument, ensuring that all necessary information is self-
contained, regardless of the possibility of external
links. These issues were resolved by embedding this
information within the document to guarantee com-
pleteness and preserve the integrity of the signed doc-
ument.
Thus, what were previously external references
and hyperlinks are transformed into self-references at
other points within the JSON object. All necessary in-
formation in the file ensures that the document is self-
contained and capable of providing all the required
data to generate a digital prescription. This step is
crucial, as there are instances where, in HL7 FHIR,
the information retrieved online tends to be volatile,
especially considering the high rate of updates based
on changes in the circumstances of the doctor and the
patient.
The next step to be defined is the signature stan-
dard to ensure the document’s validation in JSON.
The first consideration was JWS; however, its imple-
mentation has two issues. The first is the requirement
for header parameters that qualify the electronic sig-
nature, as qualified signatures are mandatory for med-
ication prescriptions. This necessitated a deeper ex-
ploration of JSON signatures. The JAdES standard,
created by ETSI, emerges as the most suitable for-
mat. The parameters for Claiming Signing Time and
those providing information about the certificate used
for signing are essential for qualifying the signatures
made by doctors when prescribing medications and
pharmacists when dispensing them.
The highlighted signature was chosen because it
allows verification of its validity without sharing doc-
ument information. HL7 FHIR proposes implement-
ing the DaVinci signature in its framework. While this
signature is also based on JWS, it was not selected for
use due to the greater robustness of the security of-
fered by JAdES. JAdES allows for the definition of
different levels, enabling more efficient validation of
signed documents over the long term.
With the assurance that the document to be signed
contains updated information from the moment it was
generated, the focus shifts to executing the qualified
signature. Here, the most critical parameter to con-
sider is the one that indicates when the document was
signed; thus, the sigT parameter is essential for con-
textualizing the timing of the signature. This enables
an application to generate and sign an electronic doc-
ument related to a prescription for a patient. In the
API, the credentials of the doctor or pharmacist are
validated before recording a prescription or dispens-
ing. The architecture diagram of the project in Figure
2 illustrates how the applications are interconnected.
Figure 2: Architecture diagram of the project.
The Signature Validator API was developed to
create the adapted FHIR document and perform se-
mantic validation of the information in the signature.
In the prescription, this API is responsible for match-
ing the doctor’s social security number (CPF) with the
number of CPF registered with a consult on the CFM
database of this doctor’s CRM number. All this pro-
cess is done when the doctor requests the API to sign
the document. This process is crucial to prevent peo-
ple who are not qualified doctors from prescribing any
medication to a third person.
The signed prescription must be valid according to
the Brazilian Pattern of Digital Signatures (PBAD) to
be accepted. A Signer API was developed to ensure
the signature is valid with PBAD and confirm that it
will be trusted and valid in Brazilian territory. This
API will create a signature with valid parameters us-
ing the certificate uploaded by the doctor in the user
interface to sign the document. It will also confirm
whether the certificate and its trust anchor are valid,
according to PBAD.
After creating and validating the prescription, the
Signature Validator API is also responsible for creat-
ing the prescription register in a database. To insert
HEALTHINF 2025 - 18th International Conference on Health Informatics
840
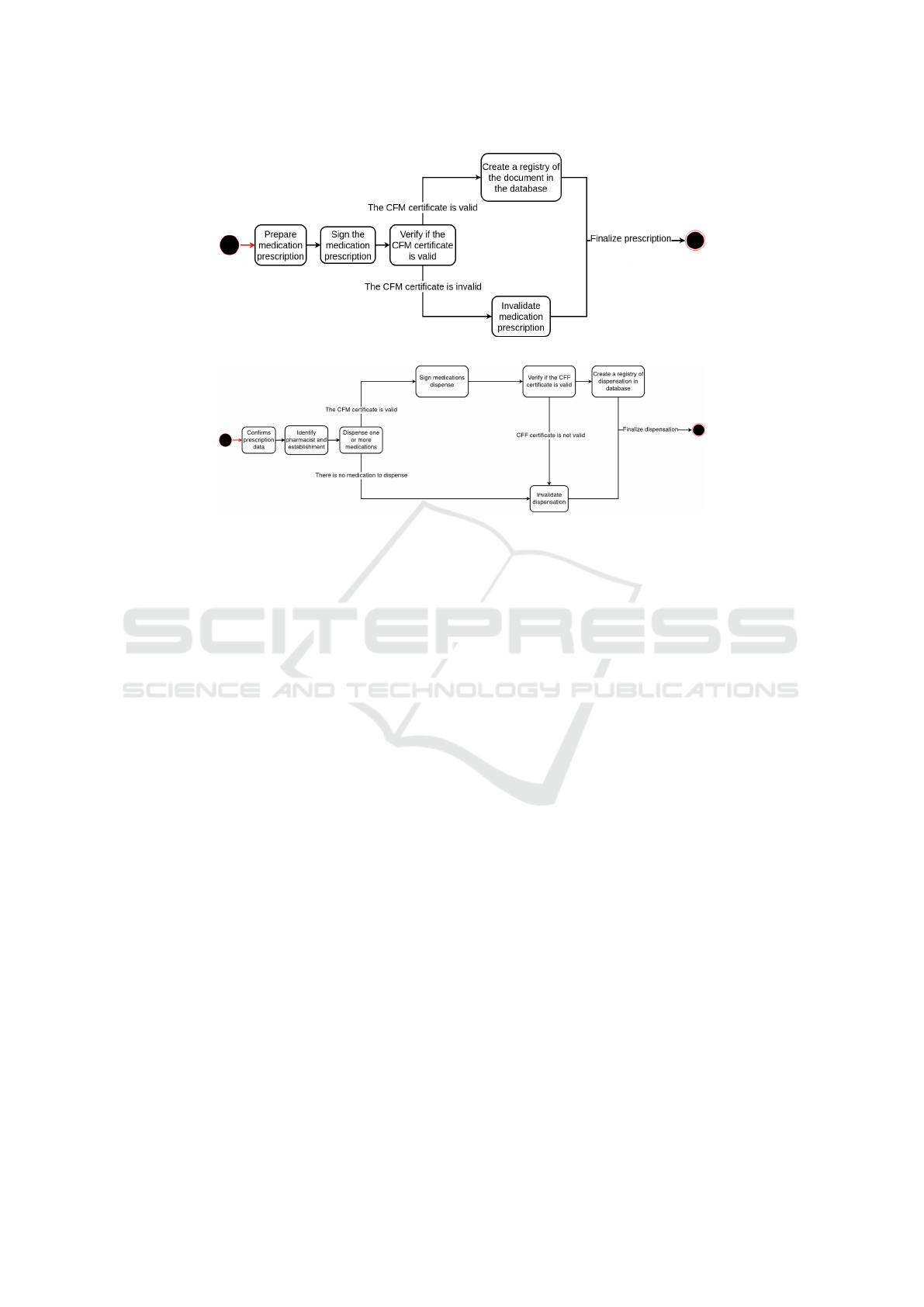
Figure 3: State machine diagram of a registry of medication prescription.
Figure 4: State machine diagram of a registry of medication prescription.
the prescription information into the database, a hash
value for each prescription is made with the date it
was created. It also creates a table with the prescrip-
tion ID and available medications to be consulted in
the dispensation. In this way, the API stores the data
and the document as shown in Figure 3.
It is important to highlight that data storage was
carried out on a local test server when the research
was conducted. However, a server with shared ac-
cess across different hospitals, clinics, doctor’s of-
fices, medical centers, and pharmacies would be es-
sential to ensure the solution’s applicability in a real-
world setting. A third-party organization interested
in implementing this solution must provide the neces-
sary infrastructure to achieve this.
To dispense the prescription medications, the
pharmacist needs the prescription’s hash value and
uses it to access its information. The Signature Val-
idator API will bring the document, check if it’s cor-
rect semantically, and send it to the Conformance Ver-
ifier API. The Conformance Verifier API will check
the validity of the signature and its trust anchors and
validate the signature parameters according to PBAD
to return to the Signature Validator API, which will
perform a query at the database and return the med-
ications prescribed and their amounts. Signer and
Conformance Verifier APIs have some common im-
plementations; therefore, these implementations were
detached and called core libraries to enhance compre-
hension and make the development easier.
After this process, the Validation API is respon-
sible for consulting possible previous dispensations
linked to that prescription by ID key and performing
the same verification made in the prescription if nec-
essary. The pharmacist has two options for dispensa-
tion: partial dispensation, which will dispense some
prescribed medications, and total dispensation, which
will dispense all prescribed medications.
To perform the dispensation, the pharmacist will
select the amount of each prescribed medication and
fill out a form with his information and CFF number.
This will allow the Signature Validator API to con-
sult the CFF database. After this confirmation, the
pharmacist will select the amount to dispense. If dis-
pensing medication is not allowed anymore, previous
dispensations will show a stack trace of dispensations.
Otherwise, the document of dispensation is created,
and the pharmacist will sign it to pass through the
validation process of the Signature Validator API and
Signer API, which will be stored with its respective
prescription as seen in Figure 4.
Unit tests were developed to guarantee the correct
functionality of APIs. Tests on Signer API verify if
all needed parameters were inserted in the signature,
it also verify if the signature was made and use arte-
facts to verify the insertion of the digest algorithm pa-
rameter. The Conformance Verifier API has tests to
see the validity of the signature, non-repudiation of
the signature, its certificate chain, and the validity of
the signature parameters.
Document Validation tests verify the correctness
of the professional’s credentials and the consistency
of the signatory’s information with the data retrieved
from the CFM and CFF databases. They also ensure
Digital Medication Prescription System with JSON
841

that the credentials are included in both the prescrip-
tion and the dispensing of medications. Additionally,
tests were developed to verify the validity of the pre-
scription and dispensing and the functionality of the
database.
After implementing all unit tests, a pilot test was
conducted with one doctor to test the API’s behav-
ior during the prescribing process and a pharmacist
to test its behavior with the partial and full dispens-
ing of medicines. In this pilot, the system behavior
was tested with valid and already dispensed receipts,
valid and invalid CRM and CFF, and valid and invalid
signatures.
6 RESULTS AND CONCLUSION
The project holds great potential to improve the pre-
scription and dispensing process, and the pilot test
showed its technical viability. It can also revolution-
ize dispensing practices with a new concept of partial
dispensing, increasing patients’ flexibility in purchas-
ing their medications. The combination of FHIR stan-
dardization and digital signatures, where the JSON
format and JAdES served as crucial communication
bridges between these concepts, demonstrated a vi-
able path toward digitalizing the medication prescrip-
tion process.
In addition to the problems already faced, this ap-
proach still needs to be facilitated for common pa-
tients. For this, the solution under analysis is to use a
PDF representation for the patient that will be issued
digitally, containing a QRcode referencing the hash
of the official medication prescription and dispensing
document. The generated PDF will be signed by the
doctor upon prescription and signed by a pharmacist
upon dispensation, and the objective is to use it as a
human-readable document.
Although adaptations are necessary, the transfor-
mations implemented have been feasible and leave
room for further evolution. The technologies em-
ployed are still considered new and can be explored in
various ways. A Brazilian definition based on FHIR
can be established, allowing for a gradual transition
from current paper prescriptions to a digital format.
For future work, a real case of use with a hospital
and pharmacy needs to be done, and in case of suc-
cess, blockchain implementation for medication dis-
pensing is proposed. This technology aligns well with
the theme by leveraging the key properties of consis-
tency and information tracking. It can potentially en-
hance security and fraud prevention, which could sig-
nificantly improve the safety of prescriptions and the
dispensing of controlled medications. This technol-
ogy can also improve the performance and the scala-
bility of this solution.
REFERENCES
Bender, D. and Sartipi, K. (2013). HL7 FHIR: An agile
and RESTful approach to healthcare information ex-
change. In Proceedings of the 26th IEEE Interna-
tional Symposium on Computer-Based Medical Sys-
tems, pages 326–331. IEEE.
Cheng, A., Duda, S., Taylor, R., Delacqua, F., Lewis, A.,
Bosler, T., Johnson, K., and Harris, P. (2021). RED-
Cap on FHIR: Clinical data interoperability services.
121:103871.
Conselho Federal de Medicina (2021). Resoluc¸
˜
ao cfm
n
o
2.299/2021. https://sistemas.cfm.org.br/normas/
visualizar/resolucoes/BR/2021/2299. Acessado em:
09 jun. 2024.
Duda, S. N., Kennedy, N., Conway, D., Cheng, A. C.,
Nguyen, V., Zayas-Cab
´
an, T., and Harris, P. A. (2022).
HL7 FHIR-based tools and initiatives to support clin-
ical research: a scoping review. 29(9):1642–1653.
European Parliament and Council of the European Union
(2014). Regulation (EU) no 910/2014 of the european
parliament and of the council of 23 july 2014 on elec-
tronic identification and trust services for electronic
transactions in the internal market and repealing direc-
tive 1999/93/EC. http://data.europa.eu/eli/reg/2014/
910/oj/eng. Acessado em: 09 jun. 2024.
Georgioska, M. (2020). Application of digital signatures in
the electronic system for public procurement in repub-
lic of north macedonia.
Gruendner, J., Gulden, C., Kampf, M., Mate, S., Prokosch,
H.-U., and Zierk, J. (2021). A framework for criteria-
based selection and processing of fast healthcare inter-
operability resources (FHIR) data for statistical anal-
ysis: Design and implementation study. 9(4):e25645.
Health Level Seven International (2023). Fhir modules.
https://hl7.org/fhir/modules.html. Acessado em: 09
jun. 2024.
Ibarz, J.-C. C. (2020). Bringing JSON signatures to
ETSI AdES framework: Meet JAdES signatures.
71:103434.
Ibarz, N. (2021). Development of a tool for validating
etsi ades digital signatures as defined by the european
standard etsi en 319 102-1.
Institute, E. T. S. (2021). Electronic signatures and infras-
tructures (esi); jades digital signatures; part 1: Build-
ing blocks and jades baseline signatures.
Jones, M. B., Bradley, J., and Sakimura, N. (2015). JSON
web signature (JWS). Num Pages: 59.
Kutyłowski, M. and Bła
´
skiewicz, P. (2023). Advanced elec-
tronic signatures and eIDAS – analysis of the concept.
83:103644.
Minist
´
erio da Sa
´
ude do Brasil (2020). Rede nacional de da-
dos em sa
´
ude (rnds). https://www.gov.br/saude/pt-br/
composicao/seidigi/rnds/rnds. Acessado em: 09 jun.
2024.
HEALTHINF 2025 - 18th International Conference on Health Informatics
842

Monsen, K. A., Heermann, L., and Dunn-Lopez, K. (2023).
FHIR-up! advancing knowledge from clinical data
through application of standardized nursing termi-
nologies within HL7® FHIR®. 30(11):1858–1864.
Nurseitov, N., Paulson, M., Reynolds, R., and Izurieta, C.
(2009). Comparison of JSON and XML data inter-
change formats: A case study.
Pohls, H. C. (2015). JSON sensor signatures (JSS): End-
to-end integrity protection from constrained device to
IoT application. In 2015 9th International Conference
on Innovative Mobile and Internet Services in Ubiqui-
tous Computing, pages 306–312. IEEE.
Presid
ˆ
encia da Rep
´
ublica do Brasil (1957). Lei n
o
3.268, de
30 de setembro de 1957. http://www.planalto.gov.br/
ccivil 03/leis/l3268.htm. Acessado em: 09 jun. 2024.
Presid
ˆ
encia da Rep
´
ublica do Brasil (1960). Lei n
o
3.820, de
11 de novembro de 1960. http://www.planalto.gov.br/
ccivil 03/leis/l3820.htm. Acessado em: 09 jun. 2024.
Presid
ˆ
encia da Rep
´
ublica do Brasil (2020). Lei
n
o
14.063, de 23 de setembro de 2020.
https://www.in.gov.br/en/web/dou/-/lei-n-14.
063-de-23-de-setembro-de-2020-278574432. Aces-
sado em: 09 jun. 2024.
Roehrs, A., Da Costa, C. A., Righi, R. R., Mayer,
A. H., Da Silva, V. F., Goldim, J. R., and
Schmidt, D. C. (2021). Integrating multiple
blockchains to support distributed personal health
records. 27(2):146045822110075.
Vorisek, C. N., Lehne, M., Klopfenstein, S. A. I., Mayer,
P. J., Bartschke, A., Haese, T., and Thun, S. (2022).
Fast healthcare interoperability resources (FHIR) for
interoperability in health research: Systematic review.
10(7):e35724.
Digital Medication Prescription System with JSON
843
