
Unified Parkinson’s Disease Rating Scale Rest Tremor Score Estimation
Using the Fundamental Frequency
Beatriz Lopo Ferreira
1 a
, Virginie Felizardo
2,3 b
, Nuno Cruz Garcia
1 c
, Mehran Pourvahab
3
,
Henriques Zacarias
2,3
, Leonice Pereira
3
and Nuno M. Garcia
4
1
LASIGE, Faculdade de Ci
ˆ
encias, Universidade de Lisboa, Lisboa, Portugal
2
Instituto de Telecomunicac¸
˜
oes, Lisboa, Portugal
3
Universidade da Beira Interior, Covilh
˜
a, Portugal
4
Instituto de Biof
´
ısica e Engenharia Biom
´
edica, Faculdade de Ci
ˆ
encias, Universidade de Lisboa, Lisboa, Portugal
Keywords:
Parkinson’s Disease, Rest Tremor, Accelerometer, Fundamental Frequency, Monitoring.
Abstract:
Parkinson’s disease (PD) is a chronic, progressive and neurodegenerative disease that affects more than 10
million people worldwide. One of the cardinal symptoms of this disease is tremor, which is characterized
as an involuntary, oscillatory movement of a body part. The tremor associated with PD can be divided into
rest tremor, postural tremor, and kinetic tremor and is characterized as a regular and asymmetric tremor.
Emerging methods involve the use of data from inertial sensors to measure, analyze and quantify tremor and
other symptoms of PD. In this publication, a method for the monitoring of rest tremor scores is explored.
This method is based on the number of windows in a signal with a fundamental frequency within the rest
tremor frequency band and has potential to be applied as a support for monitoring this symptom. This method
had a 87.88% success rate for predicting rest tremor scores on the X axis of a 4 hour accelerometer signal,
establishing promising results that will be further explored in future work.
1 INTRODUCTION
Parkinson’s disease (PD) is a chronic, progressive,
and neurodegenerative disorder (de Oliveira Andrade
et al., 2020). In addition to affecting more than
10 million people worldwide, making it the second
most common neurodegenerative disorder, PD is the
fastest growing neurological disease, being estimated
that 12 million people will be diagnosed by 2010
(Shawen et al., 2020; Burq et al., 2022). This disor-
der can cause patients to feel several motor and non-
motor symptoms, with the cardinal symptoms being
bradykinesia, rigidity, and tremor (de Oliveira An-
drade et al., 2020; Huo et al., 2020).
Tremor is considered the most common move-
ment disorder and is characterized as an involun-
tary, oscillatory movement of a body part. The
tremor associated with PD is characterized as a reg-
ular asymmetrical tremor and can be rest tremor, pos-
tural tremor, or kinetic tremor. This symptom usually
manifests itself at rest and at the onset of the disease
tends to affect the hands (Zajki-Zechmeister et al.,
a
https://orcid.org/0000-0002-7437-9493
b
https://orcid.org/0000-0001-6874-3263
c
https://orcid.org/0000-0002-6371-3310
2020).
Due to the heterogeneity of PD, accurate moni-
toring and assessment of symptoms is extremely im-
portant for the continuous selection of the most ad-
equate treatment plan, as the disease progresses and
the severity of symptoms increases (Huo et al., 2020;
Smid et al., 2022). However, the golden standard
method to evaluate PD and its symptoms, the Unified
Parkinson’s Disease Rating Scale (UPDRS) (Goetz
et al., 2008), requires a professional to perform the
evaluation, leading to a low degree of objectivity, im-
partiality, and sensitivity (de Oliveira Andrade et al.,
2020). This method has a high within-subject vari-
ability and low test-retest reliability. Moreover, the
physical exams performed in the clinical evaluation
provide only a small sample of PD symptoms, which
may not accurately represent those symptoms outside
the clinic (Burq et al., 2022).
Researchers have shown the feasibility of using
data from inertial sensors, such as accelerometers and
gyroscopes, to measure, analyze, and quantify tremor
and other motor signs of PD, with accuracies from ex-
isting trials exceeding 85% for the detection of tremor
and bradykinesia (Burq et al., 2022; Shawen et al.,
2020). From these sensors, accelerometers are con-
312
Ferreira, B. L., Felizardo, V., Garcia, N. C., Pourvahab, M., Zacarias, H., Pereira, L. and Garcia, N. M.
Unified Parkinson’s Disease Rating Scale Rest Tremor Score Estimation Using the Fundamental Frequency.
DOI: 10.5220/0013364500003938
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 11th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2025), pages 312-319
ISBN: 978-989-758-743-6; ISSN: 2184-4984
Proceedings Copyright © 2025 by SCITEPRESS – Science and Technology Publications, Lda.

sidered the minimum necessary sensor for the char-
acterization of human activity, despite it not being
clear if this sensor alone is enough to characterize PD
symptoms and improve disease detection (Huo et al.,
2020).
These sensors are cost-efficient, widely available,
and don’t rely on the interpretation of an experienced
professional, making them less subjective. Nonethe-
less, due to their potential time-consuming measure-
ments and complexity, most of these devices are not
currently used for clinical or home monitoring (Zajki-
Zechmeister et al., 2020; Smid et al., 2022). More-
over, their implementation in continuous in-the-wild
monitoring is limited by the battery life and memory
capacity of the sensor devices, which may lead to in-
termittent usage and inconsistent positioning (Shawen
et al., 2020). Another challenge lies in the distinction
between symptoms, like tremor, and normal daily ac-
tivities in signals collected in uncontrolled living con-
ditions due to noise (San-Segundo et al., 2020).
There is currently a lack of established meth-
ods/models for the correlation of PD symptoms’ sen-
sor data with UPDRS scores and no commercial sys-
tems to complement clinical assessment of symptoms
(Huo et al., 2020; San-Segundo et al., 2020). Meth-
ods to evaluate PD can generally be divided into two
categories. One being machine learning models that
can use sensor data and features (typically from the
time and/or frequency domains) from that data to de-
tect the presence and severity of symptoms (Shawen
et al., 2020; San-Segundo et al., 2020). The other
methods involve the correlation of sensor data with
PD symptoms through the creation of methods based
on the physical and physiological characteristics of
symptoms (Huo et al., 2020).
Regarding the use of the fundamental frequency
for the assessment of tremor in current literature, in
(Kuosmanen et al., 2020), the authors use the fun-
damental frequency, extracted from the periodograms
obtained through the Welch’s method, to categorize
game sessions, during which data was collected, as
types of tremor. In (Bazgir et al., 2018), a short-
time Fourier transform (STFT) was implemented and
the fundamental frequency, along with other five fre-
quency domain features, were extracted. Four classi-
fiers were tested to estimate hand tremor and Naive
Bayesian achieved the highest accuracies of 89% and
almost 90% before and after feature selection, re-
spectively. The fundamental frequency was one of
the most discriminative features. In (Pierleoni et al.,
2019), a system, including a data collection device
and two detection and classification for tremor and
freezing of gait, was developed. In this system, the
authors extract several frequency domain feature, in-
cluding the fundamental frequency, and define their
own parameter to estimate tremor severity using these
features. This system achieved an accuracy of 97.7%
for tremor. Moreover, the fundamental frequency is
one of the most commonly extracted features for the
analysis of voice changes in PD(Amato et al., 2023).
In this paper, a simple method with a low com-
putational cost for the estimation of UPRDS rest
tremor scores based on the number of windows with
a fundamental frequency between 3 and 6 Hz is ex-
plored. Firstly, the dataset used and the steps to ap-
ply this method, including the preprocessing, feature
extraction, and analysis of the data, are explored in
the methods in section 2. Then the results are pre-
sented and discussed in sections 3 and 4, respectively.
This last section also includes a brief discussion of
the dataset and the periodograms obtained with the
Welch’s method.
2 METHODS
In this section, the dataset and the method proposed
and implemented to estimate the rest tremor score at-
tributed to each individual using the UPDRS are pre-
sented.
2.1 Dataset
Due to a lack of time and resources needed to col-
lect a dataset of tremor data, an open-source dataset
collected by the authors of (Adams et al., 2021) was
used for the implementation of this framework. This
dataset contains accelerometer data from 34 individ-
uals, 17 people with Parkinson’s disease (PwPD) and
17 HC, collected at a sampling rate of 31.25 Hz using
5 lightweight MC 10 BioStamp RC sensors, placed
on the trunk, left and right anterior thighs, and left
and right anterior forearms. The data collection began
during a UPDRS clinical evaluation, performed dur-
ing the ON and OFF states of medication, and lasted
around two days.
Only the data collected from the anterior fore-
arms was used, since the study was focused on tremor
from the upper extremities. Additionally, for the in-
dividuals with ID 7 and ID 60, the dataset only con-
tains files from the sensor on the right forearm. This
dataset also contained demographic data, annotations
from the UPDRS evaluations, and clinical assessment
data, which includes the scores attributed to the rest
tremor of each individual during the evaluation. De-
mographic data and the rest tremor score given to the
anterior forearms of each individual during the ON
medication state are presented in table 1.
Unified Parkinson’s Disease Rating Scale Rest Tremor Score Estimation Using the Fundamental Frequency
313
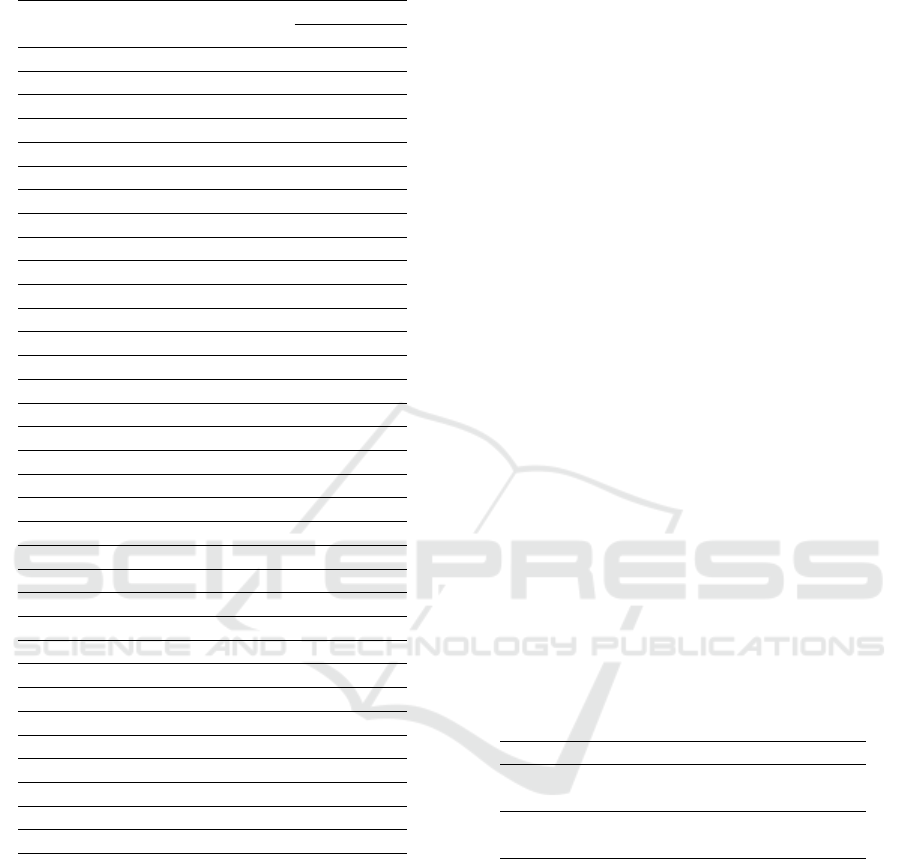
Table 1: Demographic and clinical data during the ON med-
ication state of individuals in the dataset.
ID Group Gender Age
RT score
left right
5 Control F 74 0 0
6 PD M 73 2 0
7 Control F 52 0 0
8 Control F 77 0 0
10 PD F 72 0 2
12 PD F 64 1 1
13 PD F 60 0 0
14 Control F 56 0 0
15 PD M 65 0 1
16 Control F 62 0 0
17 PD M 74 0 3
18 Control F 66 0 0
20 Control F 68 0 0
22 Control M 68 0 0
23 PD F 68 0 2
24 PD M 62 0 0
25 PD F 72 0 1
27 Control F 54 0 0
30 Control F 68 0 0
33 PD M 46 0 0
35 PD M 67 2 0
36 PD M 69 3 0
38 PD M 78 1 0
39 Control F 74 0 0
40 PD F 75 1 0
41 Control M 75 0 0
42 PD M 84 0 0
43 Control F 69 0 0
44 PD F 63 0 0
45 Control M 64 0 0
58 Control M 39 0 0
60 Control F 65 0 0
62 Control F 56 0 0
63 PD M 37 0 1
The study focused on the evaluation of rest tremor
in-the-wild with free-living conditions. Other types
of tremor, like postural tremor or kinetic tremor, were
not evaluated since the dataset only contains the UP-
DRS scores attributed during the clinical evaluation
for this type of tremor.
From each forearm of each subject, a time period
of four hours was selected from the respective data
file. This interval starts five minutes after the end of
the clinical evaluation, known through the timestamps
in the annotations. Thus giving a five minute time
margin to guarantee no data from the clinical evalua-
tion is included in the selected data. Since the eval-
uation ended on the ON medication state, the patient
is considered to be in that state for the selected four
hours. The rest tremor scores attributed to the subjects
for that medication state are shown in table 1.
2.2 Preprocessing
Firstly, the magnitude of the accelerometer signal for
the selected interval was calculated with the square
root of the sum of squares of each axis. Given that
the dataset has a sampling frequency of 31.25 Hz, no
downsampling step was implemented.
A 4
th
order high-pass Butterworth filter with a cut-
off frequency of 0.5 Hz was applied to the axes and
the magnitude vector to remove the effects of gravita-
tional acceleration and low-frequency noise.
Lastly, the axes and magnitude vector of the se-
lected data were segmented into 10 second windows,
with no overlap. This 10 second interval allows the
averaging of periodograms of segments from these
windows performed for the Welch’s method. Due to
the averaging of periodograms, the lack of overlap be-
tween the windows is also important for the correct
implementation of the Welch’s method. This method
is better described in subsection 2.3.
2.3 Feature Extraction
The features extracted in this study belonged to the
frequency domain or time domain. These features
were extracted from each of the axes and the mag-
nitude vector and are shown in table 2.
Table 2: Features extracted from the frequency and time
domains.
Domain Features
Frequency AUC, pv, F0, F50, SF50,
and |F50 − F0|
Time RMS, range, mean, variance,
skewness, and kurtosis
The frequency domain features were extracted
from the PSD. The PSD was estimated using the
Welch’s method, which is used to determine the
power contained in a signal’s frequency components
(Kuosmanen et al., 2020). To apply this method, the
data from each 10 second window was divided into
four 2.5 second segments with an overlap of 50%. Af-
terwards the periodogram of each segment was calcu-
lated and all the periodograms in each 10 second win-
dow were averaged (Welch, 1967). The periodograms
are briefly explored in section 4.2.
The frequency domain features extracted from the
averaged periodograms were the area under the curve
(AUC) between the frequencies of 3 and 6 Hz, peak
ICT4AWE 2025 - 11th International Conference on Information and Communication Technologies for Ageing Well and e-Health
314

value (pv), fundamental frequency (F0), central fre-
quency (F50), frequency dispersion (SF50), and the
absolute value of the difference between F50 and F0
(|F50 − F0|). These features were the same as the
features extracted by (Kuosmanen et al., 2020). The
AUC was computed between the frequencies of 3 Hz
and 6 Hz using the trapezoidal rule. This feature was
calculated between these frequencies to determine the
power of the signal in the interval corresponding to
the rest tremor frequencies. The features extracted
from this domain are described in table 3. The time
domain features extracted were the root mean square
(RMS), range, mean, variance, skewness, and kur-
tosis. Despite extracting features from both the fre-
quency and time domains, only features from the fre-
quency domain were explored in this study.
2.4 Data Analysis
Since rest tremor is normally observed in the between
the frequencies of 3 and 6 Hz, the windows where
the fundamental frequency (F0) is in that frequency
band were selected. It can be assumed that the se-
lected windows contain the features when, if present,
rest tremor is the dominant type of tremor.
We noticed an increase in the amount of windows
with F0 between 3 and 6 Hz as the scores increased.
For this reason, the data was analyzed regarding the
number of windows that were selected in the 4 hour
time interval, previously selected in the preprocess-
ing. That number of windows was then correlated to
the UPDRS rest tremor score. After that number was
counted for X, Y, and Z axes and the magnitude of
both forearms of each subject, the mean of the three
axes was calculated. The 4 hour intervals were di-
vided into two intervals of 2 hours and four intervals
of 1 hours and the same analysis was also performed
for those intervals.
The values of the number of windows that corre-
spond to each tremor score were defined and are pre-
sented in table 4. The values for the intervals of 2
hours and 1 hour were adapted from the values for the
4 hour interval. Since no subject in this dataset had
a rest tremor score of 4 from the clinical evaluation,
this score was excluded from the analysis.
The number of windows can be divided by 200,
100, and 50 for the 4, 2, and 1 hour intervals, respec-
tively, to get the final UPDRS score prediction, since
these values represent the number of windows in each
interval corresponding to a score for their respective
time interval, like shown in table 4. The values ob-
tained from this division were rounded down to get
the final score prediction.
3 RESULTS
In this section the results obtained for the data analy-
sis method proposed to estimate the rest tremor score
attributed to subjects during a UPDRS clinical evalu-
ation are presented.
The increase of the number of windows with the
increase in rest tremor score can be verified in table
5. This table displays, for the X axis of the 4 hour
interval, the number of instances when the data from
a forearm of any subject was attributed each score (Nº
samples), the mean number of windows, and the mean
predicted score, before rounding the prediction val-
ues, for each real score. For the samples that were
evaluated, the mean number of windows increases
with the increase of the real rest tremor score, for all
scores except score 3. Furthermore, the same increase
can be seen in the mean prediction value, except for
score 3. Excluding this last score, all mean values for
both the number of windows and the prediction are
within the established values for a correct prediction.
Table 6 contains the results for the UPDRS rest
tremor scores predictions with the number of win-
dows with F0 between 3 Hz and 6 Hz for patient 6.
This table does not include the final rounded predic-
tion values that were obtained through the division of
the number of windows by 200.
The tremor scores rounded down predictions and
the rest tremor from the clinical evaluation for patient
6 in the 4 hour time period are shown in table 7. In
this case, all predictions failed for the right forearm
and the only failed prediction for the left forearm was
in the Y axis.
This method’s success rate was determined based
on the percentage of times the prediction was correct.
The success rates for the X, Y, and Z axes, the magni-
tude, and the mean in the 4, 2, and 1 hour time inter-
vals are shown in table 8. The X axis had the highest
success rate for the 4 and 2 hour time intervals and the
Z axis had the highest success rate for the 1 hour inter-
val. Despite this, the difference between the success
rate of these axes for the later time interval was only
0.38%. Furthermore, the X axis had the overall high-
est success rate for the 4 hour interval, with 87.88%.
Predictions using the magnitude vector failed most of
the time, with the magnitude having the worst suc-
cess rate for every interval. The second worst success
rate in every interval was obtained by the Y axis. The
mean number of windows in all axes had a higher suc-
cess rate than the Z axis in the 4 hour interval, how-
ever the X and Z axes had a higher success rate for
both the 2 and 1 hour intervals.
Unified Parkinson’s Disease Rating Scale Rest Tremor Score Estimation Using the Fundamental Frequency
315
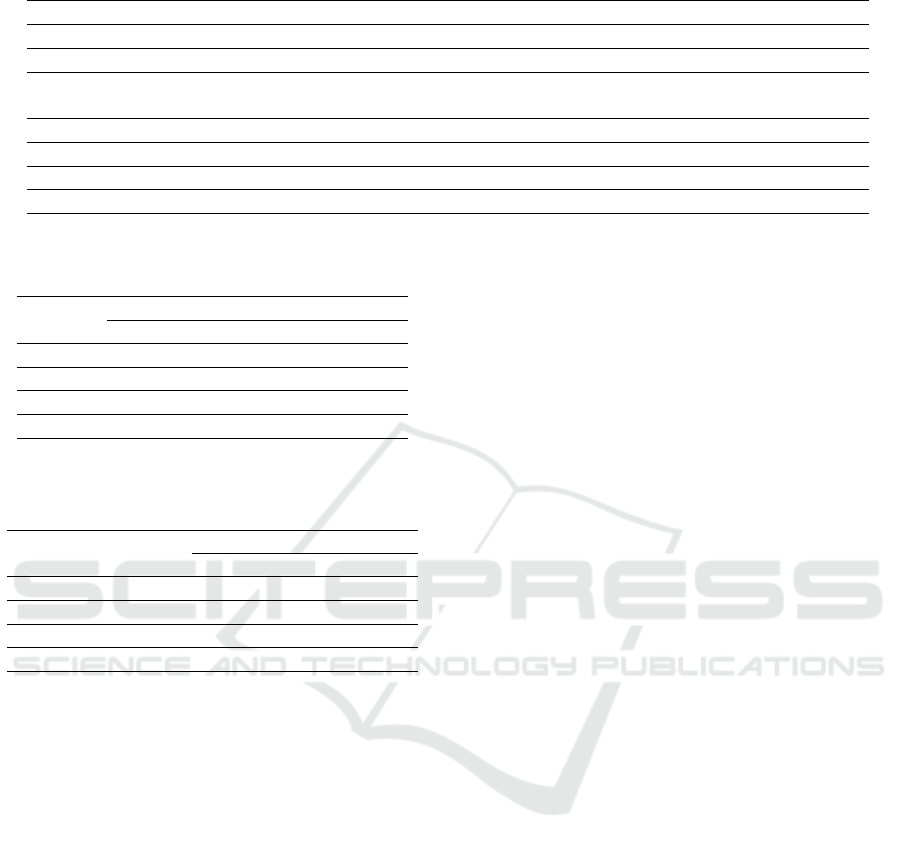
Table 3: Features extracted from the periodograms and theirs description (Kuosmanen et al., 2020).
Feature Description
AUC Total power of the signal.
pv Maximum value of the PSD.
F0 Frequency of maximum power. Can be used to determine the dominant tremor type in
a window, according to the type of tremor frequency band it belongs to.
F50 Central point where the periodograms are divided into two equal parts.
SF50 Width of the frequency band centered in F50 that contains 68% of the total power.
|F50 − F0| Absolute value of the difference between F50 and F0.
tip Calculated by dividing pv by SF50.
Table 4: UPDRS scores and the corresponding number of
windows for the 4,2, and 1 hour intervals.
UPDRS Number of windows
score 4 hours 2 hours 1 hour
0 < 200 < 100 < 50
1 200 - 400 100 - 200 50 - 100
2 400 - 600 200 - 300 100 - 150
3 > 600 300 - 400 150 - 200
Table 5: Number of samples, mean number of windows and
mean predictions for each real score in the X axis with the
4 hour time interval.
Real
Nº samples
Mean
score Nº windows Prediction
0 53 114.472 0.572
1 7 225.429 1.127
2 4 463.25 2.316
3 2 442.5 2.212
4 DISCUSSION
4.1 Dataset
Firstly, we discuss how the characteristics of this
dataset might have influenced the results.
The majority of the dataset is composed of sub-
jects who were given a rest tremor score of 0 the
UPDRS clinical evaluation. Furthermore, the dataset
contains only seven instances where rest tremors was
attributed a score of 1, four instances where it was
attributed a rest tremor score of 2 and two instances
where it was attributed a rest tremor score of 3. As
such, there are few samples of data where rest tremor
has a higher score of 3 or 4.
The authors of (Channa et al., 2021) consider a
sampling frequency of 100 Hz sufficient to measure
motor features related to PD due to the frequency of
tremor in the upper extremities being lower than 13
Hz. Nonetheless, despite some authors using higher
sampling frequencies, many studies consider a sam-
pling frequency of 50 Hz adequate for the detec-
tion of human activity with an accelerometer (San-
Segundo et al., 2020; Kuosmanen et al., 2020; Sigcha
et al., 2021). However, the sampling frequency of this
dataset is 31.25 Hz, being lower than what is typically
used in other studies.
4.2 Welch’s Periodograms
A brief visual analysis, presented in this subsection,
was performed on the PSD plots obtained from the
Welch’s method. The plots show the periodogram of
all windows in the respective axes or magnitude.
The periodograms from the left forearm of patient
5 (HC group; UPDRS rest tremor score 0 for left and
0 for right) are shown in figure 1. The majority of
peaks in these periodograms are between 0 and 3 Hz,
which is typically not associated with PD’s tremor.
The authors of (Kuosmanen et al., 2020) considered
that dyskinesia is observed in this frequency band,
in (San-Segundo et al., 2020) this frequency band
is associated with normal human movement, and in
(Shcherbak et al., 2023) the frequency band between
1 and 3 Hz is associated with bradykinesia. In addi-
tion, when subjects from the PD group have a UPDRS
rest tremor score 0, their periodograms have similar-
ities with the periodograms of subjects from the HC
group.
Figure 2 shows the periodograms from the right
forearm of patient 12 (PD group; UPDRS rest tremor
score 1 for left and 1 for right), where more plots with
peaks in the rest tremor frequency band between 3 and
6 Hz can be seen, especially on the Y axis.
In figures 3 and 4, the periodograms of the right
forearm of patient 17 (PD group; UPDRS rest tremor
score 0 for left and 3 for right) and the left forearm
of patient 36 (PD group; UPDRS rest tremor score 3
for left and 0 for right), respectively, are shown. It
was noted that, for the two instances of UPDRS rest
tremor score 3, the periodogram displayed distinctive
peaks in the rest tremor, postural tremor, and kinetic
tremor frequency bands. In the existing literature, dif-
ICT4AWE 2025 - 11th International Conference on Information and Communication Technologies for Ageing Well and e-Health
316
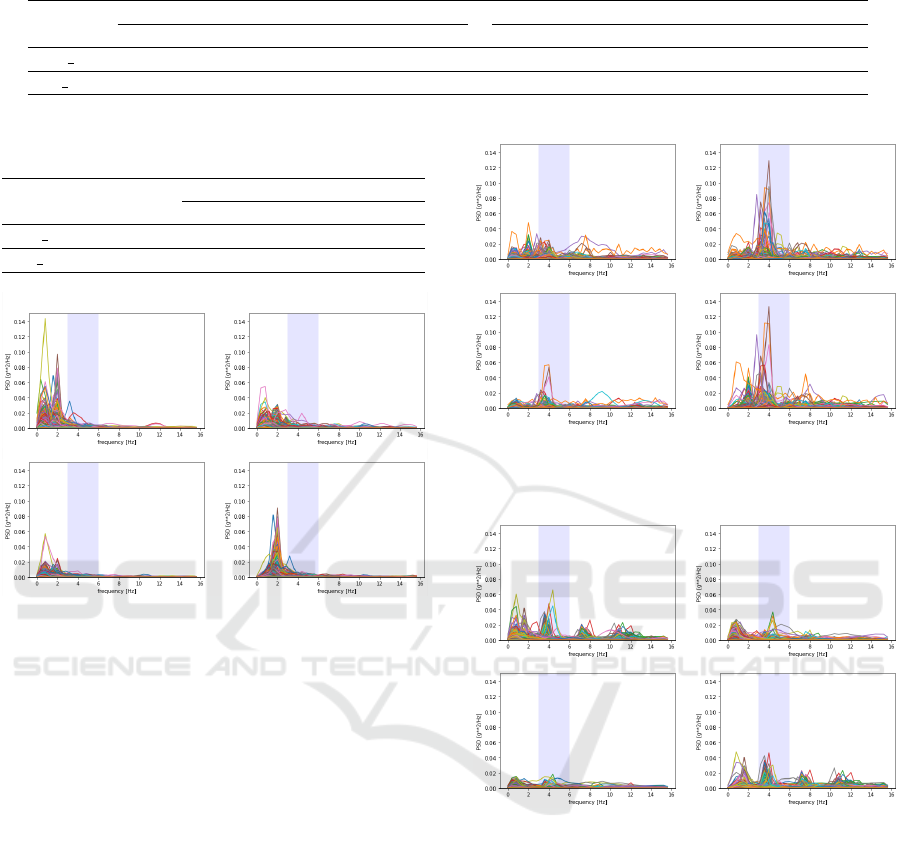
Table 6: Analysis and prediction performed on the data on both forearms of patient 6 for the 4 hour time period.
ID
Number of windows Prediction
X Y Z Magnitude Mean X Y Z Magnitude Mean
P6 left 537 297 488 436 440.67 2.68 1.48 2.44 2.18 2.20
P6 right 263 213 239 317 238.33 1.32 1.065 1.195 1.585 1.19
Table 7: Predicted and real UPDRS rest tremor scores for
patient 6 in a 4 hour time period.
ID
UPDRS Prediction
score X Y Z Mag Mean
P6 left 2 2 1 2 2 2
P6 right 0 1 1 1 1 1
Patient 5 - Left
X Y
Z Mag
Figure 1: Welch’s periodogram for the X, Y, and Z axes and
magnitude (Mag) from the left forearm of patient 5.
ferent authors tend to use different frequency bands
for the types of tremor, despite using similar values.
The frequency bands considered for this study were
between 3 and 6 Hz for rest tremor, between 6 and 9
Hz for postural tremor, and between 9 and 12 Hz for
kinetic tremor.
Some of the plots from data associated with a
tremor score 2 had similar peaks in the tremor fre-
quency bands, like in figure 5. Since no periodograms
from subjects of the HC group, who only had scores
of 0, had similar peaks, these types of plots could be
associated with PwPD and/or a higher UPDRS rest
tremor score.
All graphs in this subsection have the same PSD
axis scale, except for the periodograms of patient 36,
shown in figure 4. This was because the bigger scale
used for patient 36, whose periodograms, especially
on the Y axis, had peaks with higher PSD values,
didn’t allow the peaks in the periodograms of other
patients to be visible.
Patient 12 - Right
X Y
Z Mag
Figure 2: Welch’s periodogram for the X, Y, and Z axes and
magnitude (Mag) from the right forearm of patient 12.
X Y
Z Mag
Patient 17 - Right
Figure 3: Welch’s periodogram for the X, Y, and Z axes and
magnitude (Mag) from the right forearm of patient 17.
4.3 Data Analysis
For this dataset and the data that was evaluated, the
X axis achieved the best results in the prediction of
UPDRS rest tremor scores with the proposed method.
The discrepancies in the mean number of windows
and mean prediction for the real score 3 in table 5 can
be due to the low amount of samples for this score.
Furthermore, for the two instances where the data was
associated with a UPDRS rest tremor score 3, this
method classified one instance correctly and failed in
the other, predicting a rest tremor score 1. This may
explain the lower mean number of windows and mean
prediction than expected.
In table 7, all predictions failed for the right fore-
Unified Parkinson’s Disease Rating Scale Rest Tremor Score Estimation Using the Fundamental Frequency
317
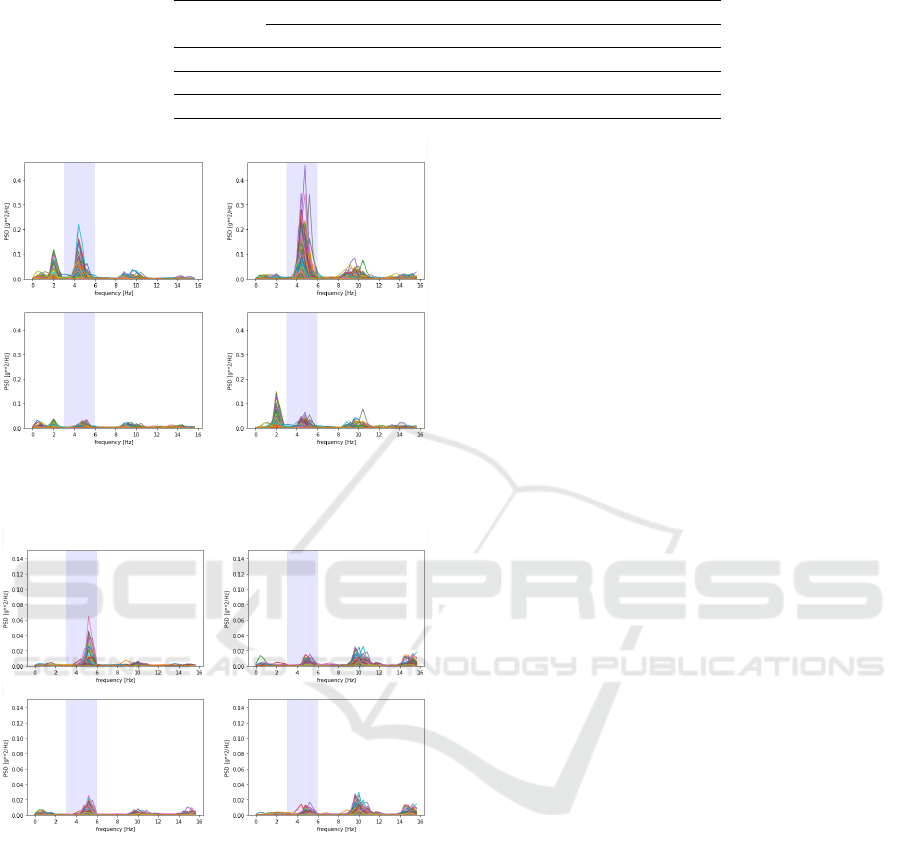
Table 8: Success rate for all axes, the magnitude and the mean of the number of windows in the 4, 2, and 1 hour intervals.
Interval
Success rate
X Y Z Magnitude Mean
4 87.88% 71.21% 81.82% 34.85% 83.33%
2 82.58% 59.09% 81.82% 37.88% 78.79%
1 77.27% 59.09% 77.65% 39.39% 74.24%
X Y
Z Mag
Patient 36 - Left
Figure 4: Welch’s periodogram for the X, Y, and Z axes and
magnitude (Mag) from the left forearm of patient 36.
X Y
Z Mag
Patient 6 - Left
Figure 5: Welch’s periodogram for the X, Y, and Z axes and
magnitude (Mag) from the left forearm of patient 6.
arm. It is possible that, since the amplitude of tremor
and consequently its tremor score can vary during the
day, no tremor was present during the evaluation, but
it was present during the 4 hour time period that was
evaluated. Moreover, another possibility is that noise
in the signal might have affected these predictions.
The prediction values were rounded down to ob-
tain the final score predictions, however the analysis
of the values with decimals allows us to know how
close the prediction was to the limit between scores
and by how much it failed. If all windows for the X
axis in the 4 hour time period (which had the high-
est success rate) that failed the prediction by less than
0.1 were discarded, the success rate would increase to
92.06%. Nonetheless, discarding only the windows
with a failed prediction is not feasible in the imple-
mentation of this method in a real setting where it is
not known which predictions are correct or incorrect.
If all windows within 0.1 of the limit between scores
were discarded and their prediction was marked as in-
conclusive between the two scores they are closest to,
a success rate of 91.23% would be achieved. Further-
more, the indication of which scores the inconclusive
prediction is in between could be helpful in a clini-
cal setting, helping the specialist know what were the
closest scores to the prediction. For example, win-
dows with values between 0.9 and 1, including these
values would be discarded and marked as inconclu-
sive between the scores 0 and 1.
It is important to note that tremor may not be con-
stantly present and its amplitude can vary during the
day. As such, the connection between the number of
windows with F0 within 3 and 6 Hz and the UPDRS
rest tremor score could lie in a potential connection
between the rest tremor amplitude (referred to as rest
tremor score in this study) and the constancy of rest
tremor. This possible connection should be further
explored in future work. The results in this study may
have also been affected by noise, due to evaluation
in free-living and in-the-wild conditions, and the low
number of samples for the UPDRS rest tremor scores
2 and 3. The number of window intervals correspond-
ing to which score were loosely established to explore
this method and could be improved in future work.
However, the method shows promising results, which
could be further improved by refining the number of
windows intervals corresponding to each rest tremor
score, as previously mentioned, and other parts of the
method.
5 CONCLUSIONS
This study is focused on the rest tremor associated
with Parkinson’s disease and the estimation of its rest
tremor score according to the UPDRS using data from
accelerometers. In this paper we explore a method
based on the number of windows in a signal where the
fundamental frequency (F0) is in the rest tremor fre-
quency band, indicating that, when present, the dom-
ICT4AWE 2025 - 11th International Conference on Information and Communication Technologies for Ageing Well and e-Health
318

inant type of tremor is the rest tremor. This method
to estimate the rest tremor scores had promising re-
sults and has a low computational cost. After being
further explored and refined, this method has the po-
tential of being implemented for the clinical support
of rest tremor evaluation, helping monitor rest tremor
and the progression of the disease by providing data
for follow-up consultations. This method is limited by
the use of tremor scores given during the clinical eval-
uation in a controlled environment as labels for data
collected in free-living, which can lead to some data
being incorrectly labeled. Thus, the method should be
tested with other datasets to verify its results and with
sensor data collected during the clinical evaluations,
helping validate the method to be applied in a con-
trolled environment. Moreover, the results shown the
capability of this feature in the assessment of tremor
and its use with classical machine learning or deep
learning models for this task should be further ex-
plored.
REFERENCES
Adams, J. L., Dinesh, K., Snyder, C. W., Xiong, M.,
Tarolli, C. G., Sharma, S., Dorsey, E. R., and Sharma,
G. (2021). A real-world study of wearable sen-
sors in parkinson’s disease. npj Parkinson’s Disease,
7(1):106.
Amato, F., Saggio, G., Cesarini, V., Olmo, G., and Costan-
tini, G. (2023). Machine learning-and statistical-based
voice analysis of parkinson’s disease patients: A sur-
vey. Expert Systems with Applications, 219:119651.
Bazgir, O., Habibi, S. A. H., Palma, L., Pierleoni, P., and
Nafees, S. (2018). A classification system for assess-
ment and home monitoring of tremor in patients with
parkinson’s disease. Journal of Medical Signals &
Sensors, 8(2):65–72.
Burq, M., Rainaldi, E., Ho, K. C., Chen, C., Bloem,
B. R., Evers, L. J. W., Helmich, R. C., Myers, L.,
Marks, W. J., and Kapur, R. (2022). Virtual exam
for parkinson’s disease enables frequent and reliable
remote measurements of motor function. npj Digital
Medicine, 5(1). Cited by: 6; All Open Access, Gold
Open Access, Green Open Access.
Channa, A., Ifrim, R.-C., Popescu, D., and Popescu, N.
(2021). A-wear bracelet for detection of hand tremor
and bradykinesia in parkinson’s patients. Sensors,
21(3):981.
de Oliveira Andrade, A., Paixao, A. P. S., Cabral, A. M.,
Rabelo, A. G., Luiz, L. M. D., Dion
´
ısio, V. C., Vieira,
M. F., Pereira, J. M., Rueda, A., Krishnan, S., et al.
(2020). Task-specific tremor quantification in a clini-
cal setting for parkinson’s disease. Journal of Medical
and Biological Engineering, 40(6):821–850.
Goetz, C. G., Tilley, B. C., Shaftman, S. R., Stebbins, G. T.,
Fahn, S., Martinez-Martin, P., Poewe, W., Sampaio,
C., Stern, M. B., Dodel, R., et al. (2008). Movement
disorder society-sponsored revision of the unified
parkinson’s disease rating scale (mds-updrs): scale
presentation and clinimetric testing results. Movement
disorders: official journal of the Movement Disorder
Society, 23(15):2129–2170.
Huo, W., Angeles, P., Tai, Y. F., Pavese, N., Wilson, S.,
Hu, M. T., and Vaidyanathan, R. (2020). A heteroge-
neous sensing suite for multisymptom quantification
of parkinson’s disease. IEEE Transactions on Neural
Systems and Rehabilitation Engineering, 28(6):1397–
1406.
Kuosmanen, E., Wolling, F., Vega, J., Kan, V., Nishiyama,
Y., Harper, S., Van Laerhoven, K., Hosio, S., Fer-
reira, D., et al. (2020). Smartphone-based monitor-
ing of parkinson disease: quasi-experimental study to
quantify hand tremor severity and medication effec-
tiveness. JMIR mHealth and uHealth, 8(11):e21543.
Pierleoni, P., Belli, A., Bazgir, O., Maurizi, L., Paniccia, M.,
and Palma, L. (2019). A smart inertial system for 24h
monitoring and classification of tremor and freezing
of gait in parkinson’s disease. IEEE Sensors Journal,
19(23):11612–11623.
San-Segundo, R., Zhang, A., Cebulla, A., Panev, S., Tabor,
G., Stebbins, K., Massa, R. E., Whitford, A., De la
Torre, F., and Hodgins, J. (2020). Parkinson’s dis-
ease tremor detection in the wild using wearable ac-
celerometers. Sensors, 20(20):5817.
Shawen, N., O’Brien, M. K., Venkatesan, S., Lonini, L.,
Simuni, T., Hamilton, J. L., Ghaffari, R., Rogers, J. A.,
and Jayaraman, A. (2020). Role of data measurement
characteristics in the accurate detection of parkinson’s
disease symptoms using wearable sensors. Journal of
neuroengineering and rehabilitation, 17(1):1–14.
Shcherbak, A., Kovalenko, E., and Somov, A. (2023). De-
tection and classification of early stages of parkinson’s
disease through wearable sensors and machine learn-
ing. IEEE Transactions on Instrumentation and Mea-
surement, 72:1–9.
Sigcha, L., Pav
´
on, I., Costa, N., Costa, S., Gago, M.,
Arezes, P., L
´
opez, J. M., and De Arcas, G. (2021). Au-
tomatic resting tremor assessment in parkinson’s dis-
ease using smartwatches and multitask convolutional
neural networks. Sensors, 21(1):291.
Smid, A., Elting, J. W. J., van Dijk, J. M. C., Otten, B.,
Oterdoom, D. M., Tamasi, K., Heida, T., van Laar, T.,
and Drost, G. (2022). Intraoperative quantification of
mds-updrs tremor measurements using 3d accelerom-
etry: A pilot study. Journal of Clinical Medicine,
11(9):2275.
Welch, P. (1967). The use of fast fourier transform for
the estimation of power spectra: a method based on
time averaging over short, modified periodograms.
IEEE Transactions on audio and electroacoustics,
15(2):70–73.
Zajki-Zechmeister, T., K
¨
ogl, M., Kalsberger, K., Fran-
thal, S., Homayoon, N., Katschnig-Winter, P., Wen-
zel, K., Zajki-Zechmeister, L., and Schwingenschuh,
P. (2020). Quantification of tremor severity with a mo-
bile tremor pen. Heliyon, 6(8):e04702.
Unified Parkinson’s Disease Rating Scale Rest Tremor Score Estimation Using the Fundamental Frequency
319
