Automated Performance Metrics for Objective Surgical Skill Assessment
in Laparoscopic Training
Asaf Arad
1
, Julia Leyva I Torres
1
, Kristian Nyborg Jespersen
1
, Nicolaj Boelt Pedersen
1
,
Pablo Rey Valiente
1
, Alaa El-Hussuna
2
and Andreas Møgelmose
1
1
Department of Electronic Systems, Aalborg University, Denmark
2
Open Source Research Collaboration, Aalborg, Denmark
Keywords:
Automated Performance Metrics, Laparoscopic Surgery, Multi Object Tracking.
Abstract:
The assessment of surgical skill is critical in advancing surgical training and enhancing the performance of
surgeons. Traditional evaluation methods relying on human observation and checklists are often biased and
inefficient, prompting the need for automated and objective systems. This study explores the use of Auto-
mated Performance Metrics (APMs) in laparoscopic surgeries, using video-based data and advanced object
tracking techniques. A pipeline was developed, combining a fine-tuned YOLO11 model for detection with
state-of-the-art multi-object trackers (MOTs) for tracking surgical tools. Metrics such as path length, velocity,
acceleration, jerk, and working area were calculated to assess technical performance. BoT-SORT emerged as
the most effective tracker, achieving the highest HOTA and MOTA, enabling robust tool tracking. The system
successfully extracted APMs to evaluate and compare surgical performance, demonstrating its potential for
objective assessment. This work validates state-of-the-art algorithms for surgical video analysis, contributing
to improved surgical training and performance evaluation. Future efforts should address limitations like pixel-
based measurements and dataset variability to enhance the system’s accuracy and applicability, ultimately
advancing patient safety and reducing training costs.
1 INTRODUCTION
Accurate assessment of surgical performance is a
cornerstone of surgical training, especially as the
field advances toward proficiency-based methodolo-
gies (Jin et al., 2018; Ebina et al., 2022a; Ebina et al.,
2022b; Guerin et al., 2022). Traditional methods of
evaluating trainees, which rely on human observers
and task-specific checklists, are accessible, but suf-
fer from bias and time inefficiencies (D’Angelo et al.,
2015). These limitations highlight the need for auto-
mated and objective assessment systems which pro-
vide consistent and detailed feedback to trainees.
APMs have emerged as a promising solution, of-
fering objective and data-driven evaluations as sug-
gested by Ebina et al. (Ebina et al., 2022b). By lever-
aging video-based data and computer vision tech-
niques, APMs can be used to analyze surgical perfor-
mance with higher precision and reproducibility. Un-
like traditional observer-based methods, APMs elim-
inate bias and offer a standardized approach for eval-
uating surgical skills, allowing the surgeons to po-
tentially improve upon surgical training programs
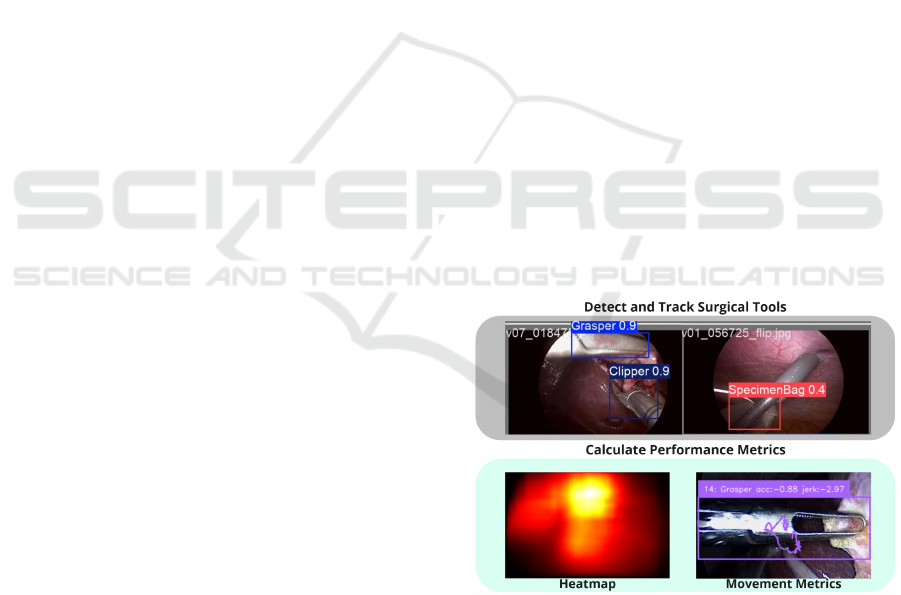
Figure 1: Simple illustration showcasing the detection of
surgical instruments used to calculate popular performance
metrics for surgical skill evaluation.
(Buckley et al., 2015; Peng et al., 2019; Sallaberry,
Tori, and Nunes, 2022).
Recent advancements in artificial intelligence,
particularly in object detection and object tracking,
have enabled the development of robust APM sys-
tems. Technologies such as Convolutional Neural
824
Arad, A., Leyva I. Torres, J., Jespersen, K. N., Pedersen, N. B., Valiente, P. R., El-Hussuna, A. and Møgelmose, A.
Automated Performance Metrics for Objective Surgical Skill Assessment in Laparoscopic Training.
DOI: 10.5220/0013380300003912
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 20th International Joint Conference on Computer Vision, Imaging and Computer Graphics Theory and Applications (VISIGRAPP 2025) - Volume 3: VISAPP, pages
824-830
ISBN: 978-989-758-728-3; ISSN: 2184-4321
Proceedings Copyright © 2025 by SCITEPRESS – Science and Technology Publications, Lda.

Networks (CNNs) allow automatic tracking and anal-
ysis of surgical instruments, providing a detailed un-
derstanding of tool usage, motion efficiency, and task
completion. These capabilities pave the way for gen-
erating a wide range of performance metrics, includ-
ing time efficiency, path consistency, and tool uti-
lization patterns, offering valuable insights for both
trainees and trainers (Twinanda et al., 2016; Jin et
al., 2018; Rivas-Blanco et al., 2021).
This work focuses on the identification and im-
plementation of common APMs for surgical perfor-
mance evaluation in laparoscopic surgeries; a mini-
mally invasive surgical method using small incisions
and a camera to guide the procedure (Rivas-Blanco et
al., 2021). Specifically, the project aims to develop a
pipeline of an image recognition system, which is ca-
pable of tracking surgical instruments and calculating
performance metrics based on their motion and usage
during procedures (Figure 1). The main contribution
of this work is validation of state-of-the-art trackers’
abilities to extract popular metrics used for evaluat-
ing surgical skills from 2D captured videos of laparo-
scopic surgeries. In future work, these metrics could
serve as a basis for comparative studies with tradi-
tional surgical skill evaluation techniques, providing
insights into their alignment with surgical expertise.
2 RELATED WORKS
When identifying the most commonly used APMs,
the following was found: Metrics such as path length
(the distance traveled by a tool), operative time (to-
tal and sub-task durations), velocity (tool movement
speed), jerk (smoothness of motion), acceleration
(rate of motion change), and tool angle (orientation
of tools) are frequently implemented for their abil-
ity to evaluate motion efficiency and skill precision
in both laparoscopic and robotic surgeries (Buckley
et al., 2015; Ebina et al., 2022b; Guerin et al., 2022).
Certain metrics, such as force measurements, are
specific to robotic surgeries due to the built-in sam-
pling of instrument sensor data, which enables pre-
cise evaluation of applied forces (Sallaberry, Tori, and
Nunes, 2022; Trejos et al., 2014). Other metrics can
also be categorized into procedure-specific metrics,
such as stitching techniques used in bladder sutur-
ing (Chen et al., 2018). Similarly, deep features ex-
tracted via deep learning approaches can be consid-
ered a separate category (Jin et al., 2018; Reiley et al.,
2011; Rivas-Blanco et al., 2021; Moglia et al., 2021).
Figure 2 summarizes the 10 most commonly used
APMs, according to an unstructured literature review
conducted by us, based on 26 relevant papers found
through Google Scholar and PubMED using the key-
words Automatic Performance Metrics AND (Surgery
OR Surgery Training) and Objective Evaluation AND
(Surgery OR Surgery Training).
Figure 2: Table showcasing the 10 most popular perfor-
mance metrics found, ordered by most frequently found
(left) to least frequently found (right).
The majority of popular APMs rely on tracking
surgical tools, often through video data, to provide the
positional and motion information needed for perfor-
mance evaluation. However, tool tracking in surgi-
cal environments is challenging due to factors such as
low-texture organ surfaces, visual artifacts from fluids
or reflections, and dynamic environmental conditions
like blood or smoke (Schmidt et al., 2024).
3 METHODOLOGY
The methodology for this project was designed to de-
velop a comprehensive pipeline for assessing surgi-
cal performance. The process involves the detection,
tracking, and analysis of surgical tools within laparo-
scopic videos, as illustrated in Fig. 3.
The workflow begins with video input of surgical
procedures, where the tools used need to be detected
and localized. A YOLO11 object detection model,
was fine-tuned on a surgical tool dataset to detect the
tools’ bounding boxes in each frame. The detected
bounding boxes were then passed to state-of-the-
art MOTs to establish temporal consistency between
frames. The selection of the most suitable tracker was
based on MOT metrics such as HOTA, MOTA, and
IDF1. The tracked tools’ motion data, including path
length, velocity, acceleration, jerk, and working area,
were then aggregated into APMs. These metrics were
compiled into an output table, facilitating compara-
tive analysis of surgical videos and providing possible
Automated Performance Metrics for Objective Surgical Skill Assessment in Laparoscopic Training
825
insights into the performance of these procedures.
Input video of
surgical procedure
Detection and
localization of
surgical tools
YOLO11 model
fine-tuned
on surgical
tool dataset
Extract APMs
from tracked tools
Tracker chosen
based on MOT
metrics (HOTA,
MOTA, IDF1)
Output table
containing APMs
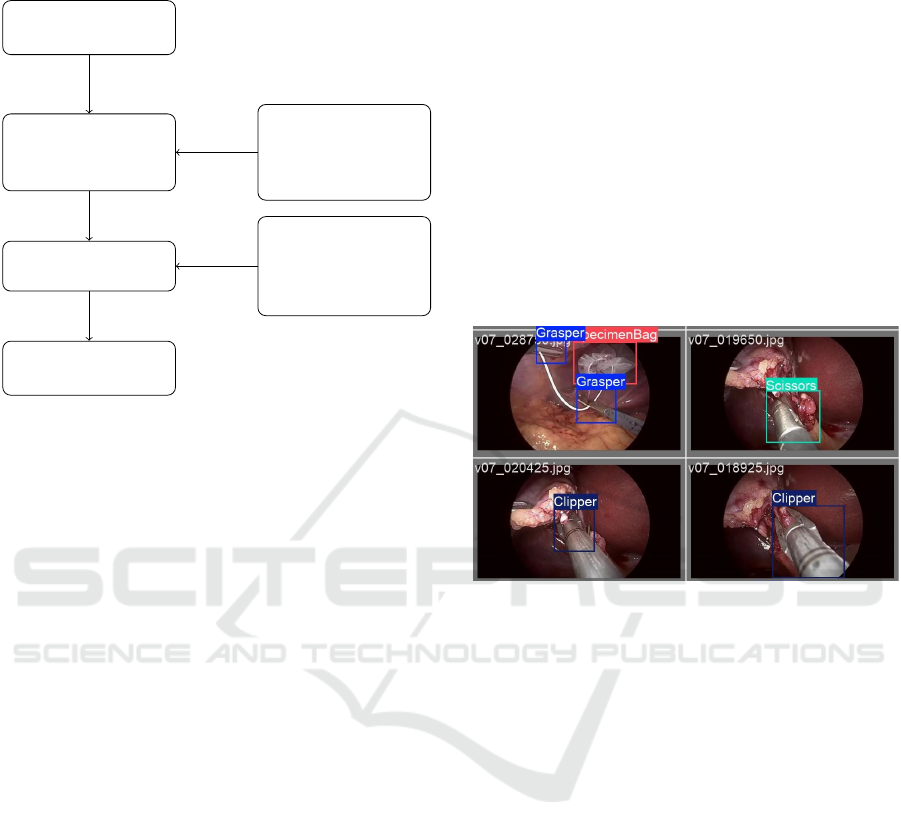
Figure 3: Flow Chart of the steps for extracting APMs from
surgical videos.
3.1 Identifying State of the Art Trackers
Three state-of-the-art MOTs have been identified and
implemented: BOT-SORT, ByteTrack, and UniTrack.
These three trackers were selected based on their good
performance on benchmarks from (Benchmark", n.d.)
and (Code", n.d.).
• BOT-SORT enhances the Simple Online and Re-
altime Tracking (SORT) framework with im-
proved Kalman filtering, camera motion com-
pensation, and a combination of Intersec-
tion over Union (IoU) and Re-Identification
(ReID) (Aharon, Orfaig, and Bobrovsky, 2022).
• ByteTrack leverages low-confidence detections to
recover missed objects, using a two-step associa-
tion process (Zhang et al., 2022).
• UniTrack employs a unified model for multiple
tracking tasks and uses reconstruction-based sim-
ilarity for better associations (Wang et al., 2021).
3.2 Tracker Evaluation
To evaluate the trackers, MOT metrics have been cal-
culated, including Higher Order Tracking Accuracy
(HOTA), Multi-Object Tracking Accuracy (MOTA),
and Identity F1 (IDF1) for each tracker. These evalu-
ation metrics quantify how well the trackers perform
on a given data set. MOTA prioritizes detection (iden-
tification and localization) accuracy, IDF1 prioritizes
association (maintaining the identity of objects be-
tween frames) accuracy, and HOTA was created to
balance the accuracy of both detection and associa-
tion to align with human perception (J Luiten., 2021).
3.3 Datasets
The dataset was employed by a combination of pub-
licly available datasets from laparoscopic videos.
The dataset used for model training is m2cai16-tool-
locations (Jin et al., 2018), which includes 2,532
frames annotated with bounding box coordinates for
seven surgical tools (Grasper, Bipolar, Hook, Scis-
sors, Clipper, Irrigator and Specimen Bag). This
dataset was chosen because of its detailed annotations
and diversity of tool types, which facilitated robust
model training. Examples are shown in figure 4.
Figure 4: Frame examples of m2cai16-tool-locations
dataset.
For testing the trackers’ performance, we used
the Cholec80-Boxes dataset (Abdulbaki Alshirbaji et
al., 2024), which contains annotations at 1 fps for 5
videos from Cholec80 (Twinanda et al., 2016). As op-
posed to m2cai16-tool-locations, this dataset contains
sequential frames arranged in chronological order.
3.4 Fine Tuning Using YOLO11
As all the identified trackers use YOLO for object de-
tection, a YOLO model was fine-tuned to adapt it in
our domain. For this, YOLO11 was chosen as it is the
latest, and best performing, version at the time of writ-
ing (Jocher and Qiu, 2024). The model was fine-tuned
exclusively with the m2cai16-tool-locations dataset
using a dataset split of 70%/15%/15% (Training, val-
idation, test).
For fine-tuning, the medium model, YOLO11m,
was chosen, as it has a good trade-off between com-
plexity and performance. The model was trained for
500 epochs using the default hyperparameters pro-
vided by Ultralytics (Jocher and Qiu, 2024).
Figure 5 illustrates the training and validation loss
across the epochs, stopping at epoch 215 due to early
VISAPP 2025 - 20th International Conference on Computer Vision Theory and Applications
826
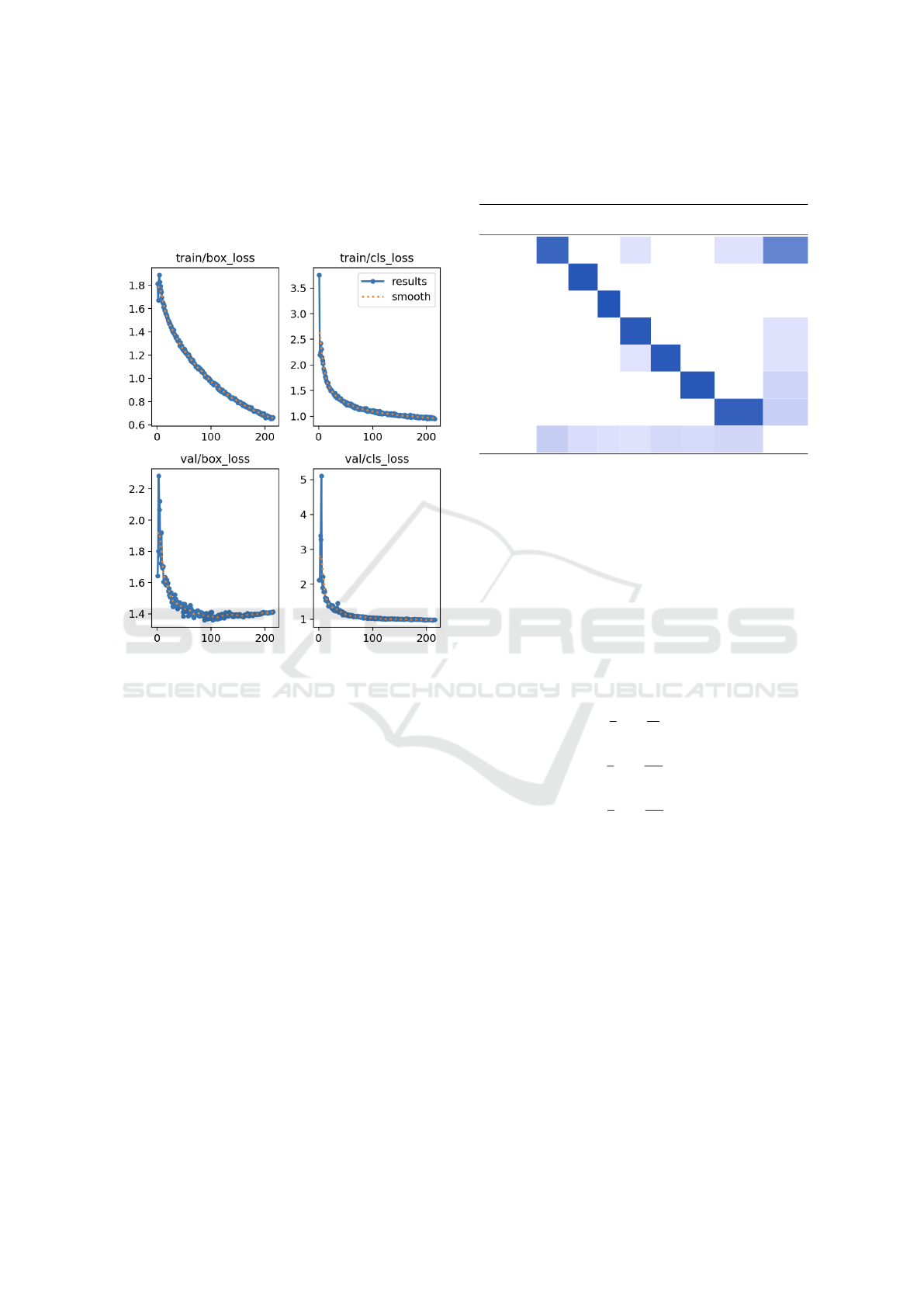
stopping. The model achieved its best performance at
epoch 115, with a box validation loss of 1.38 and a
CLS validation loss of 1.01. The corresponding pre-
cision and recall scores were 0.48 and 0.91, respec-
tively.
Figure 5: Training/Validation loss (Y-axis) of the fine-tuned
YOLO model for each epoch (X-axis).
Testing the model on the remaining 15% of the
data resulted in a mean average precision (mAP@0.5)
of 0.957 across all classes, with the Hook class
achieving the highest mAP@0.5 (0.992), and the
Grasper class achieving the lowest mAP@0.5 (0.896).
Table 1 shows the confusion matrix of our classifica-
tion model where columns represent the true classes
and rows the prediction. The lowest detection score
was observed for the Grasper, which was misclassi-
fied as background in 0.16% of cases. However, it
is worth noting that the Grasper appeared far more
frequently in the dataset (223 instances) compared
to the other classes Bipolar (72), Hook (49), Scis-
sors (66), Clipper (48) Irrigator (57), and Specimen
Bag (77). Generally, the classification errors primar-
ily stem from missed detections as opposed to confu-
sion between the classes.
3.5 Acquisition of APMs
In order to be able to quantitatively assess surgical
performance, the following APMs were chosen for
calculation: path length (Eq. 1), average velocity (Eq.
2), average acceleration (Eq. 3), and average jerk
Table 1: Confusion matrix for the YOLO11 test results,
highlighting which classes the model confuses with each
other.
Predicted / True Grasper Bipolar Hook Scissors Clipper Irrigator SpecimenBag Background
Grasper 0.84 0.03 0.03 0.64
Bipolar 0.94
Hook 0.96
Scissors 0.92 0.03
Clipper 0.02 0.92 0.03
Irrigator 0.93 0.12
SpecimenBag 0.87 0.15
Background 0.16 0.06 0.04 0.03 0.08 0.07 0.10
(Eq. 4). These were selected based on the most com-
monly used APMs derived from the literature search
(see 2) that we also deemed possible to calculate using
the datasets that were available. In addition, working
area (Eq. 5) can be managed as it depends only on
the object position appearance. The APMs are ac-
quired using the center of the bounding box from the
tracker results. The spatial metrics are obtained using
Savitzky-Golay smoothing filter of the position of the
tools suggested by Ebina et al. (Ebina et al., 2022b).
P L =
n−1
∑
i=1
∥p
tip
(i + 1) − p
tip
(i)∥ (1)
¯v =
1
n
n
∑
i=1
∥
d
dt
p
tip
(i)∥ (2)
¯a =
1
n
n
∑
i=1
∥
d
2
dt
2
p
tip
(i)∥ (3)
¯
J =
1
n
n
∑
i=1
∥
d
3
dt
3
p
tip
(i)∥ (4)
WA = (x
(q=97.5%)
− x
(q=2.5%)
) · (y
(q=97.5%)
− y
(q=2.5%)
)
(5)
Where p
tip
(i) represents the tool tip in frame i, and
x
(q=97.5%)
and x
(q=2.5%)
are the 97.5-percentile and
2.5-percentile, respectively, of the bounding box cen-
ter position in the X-axis, and similarly for the Y-axis.
4 RESULTS
We evaluated state-of-the-art trackers using standard
metrics (MOTA, HOTA, and IDF1). Among the
evaluated trackers, BoT-SORT achieved the highest
scores and proved to be the most effective for our
dataset. As a result, it was selected for computing
the APMs, which are used to compare the technical
Automated Performance Metrics for Objective Surgical Skill Assessment in Laparoscopic Training
827
skill and performance across different laparoscopic
surgery videos.
4.1 Trackers
Table 2: MOT metrics from BoT-SORT, ByteTrack, and
UniTrack of the videos from Cholec80-Boxes dataset.
Tracker \ Metric MOTA HOTA IDF1
BoT-SORT 54.46 12.61 9.17
ByteTrack 51.17 11.44 8.48
UniTrack 48.77 11.71 9.37
Table 2 shows the results of MOTA, HOTA and
IDF1 metrics obtained from each tracker. BoT-SORT
was selected as the main tracker due to its superior
HOTA score (12.61), reflecting its strong ability to
balance detection accuracy and trajectory association.
Although BoT-SORT only demonstrated marginally
better performance on individual metrics, it demon-
strated consistently solid performance overall. It also
achieved the highest MOTA (54.46) and performed
well in IDF1 (9.17) compared to the others. Byte-
Track, although slightly behind BoT-SORT, showed
strong performance in MOTA (51.17) but had the low-
est HOTA score (11.44). UniTrack was the best in
IDF1 (9.37) but lagged behind in MOTA and HOTA,
indicating a less balanced performance overall.
4.2 APMs
Table 3 shows the APM scores of the videos from
Cholec80-Boxes dataset. The videos have approxi-
mately the same length and were captured using the
same surgical instrument types as mentioned in sec-
tion 3.3. The chosen APMs were acquired using the
calculations in section 3.5. The scores for each video
were acquired using BoT-SORT tracking outputs for
each tool type, then the total scores were calculated
as a weighted mean of all instruments. The average
weighting was acquired using the appearance tem-
poral ratio of each tool type in the entire video, i.e.,
the ratio between the number of frames each tool ap-
peared and the total number of frames. In addition,
the path length score is represented by the total path
length per minute in each video, for scalability.
It can be observed that video04 and video02 have
the longest path length and the largest working area.
They also have the highest average velocity, acceler-
ation, and jerk, i.e. the movements in those videos
are incoherent and might often have jitter and shaki-
ness. In contrast, video05 has the shortest path length
and the smallest working area, and a smaller average
velocity, acceleration, and jerk. Thus, it might have
smoother and less shaky movements and more coher-
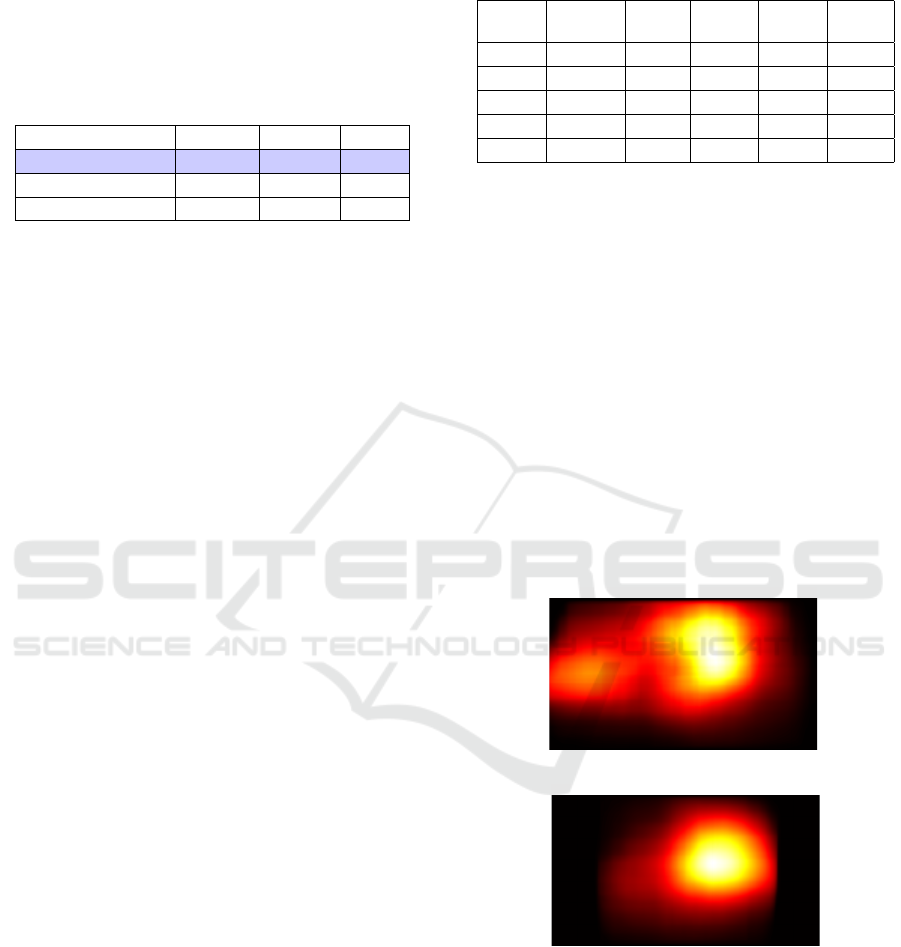
Table 3: Examples of APM calculations from different
videos.
PL
[pixel/min]
¯
v
[pixel/s]
¯
a
[pixel/s
2
]
J
[pixel/s
3
]
WA
[pixel
2
]
video01 3213 57.67 30.16 32.24 149250
video02 3771 80.86 38.38 40.43 122654
video03 1715 63.15 30.81 32.84 110318
video04 3258 65.14 36.64 39.06 147245
video05 1888 56.94 29.49 31.17 81156
ent and accurate movements during the operation.
Furthermore, in order to analyze and comprehend
the APMs acquired from tracking a video, we gener-
ate heat maps of the total number of appearances and
the locations of the surgical tools from laparoscopic
videos. Heat maps illustrate the working area metric,
and may serve as an indicator of technical skill, as it
shows how focused the surgeon is during the proce-
dure. It may leverage comparison methods between
different videos (Jin et al., 2018). Figure 6 shows ex-
amples of heat maps obtained from 2 aforementioned
tracked videos: video04 (fig. 6a) and video05 (fig.
6b). It may be deemed from the visualization of the
heat maps that video05 has more focused and accu-
rate movements, compared to video04, as matching
the comparison of the aforementioned metrics in ta-
ble 3.
Total heatmap
(a) video04.
Total heatmap
(b) video05.
Figure 6: Heat map of bounding box occurrences and loca-
tions of tools in two full laparoscopic videos.
5 DISCUSSION
In this study, we focused on automating the assess-
ment of surgical performance in laparoscopic surg-
eries by tracking surgical tools and computing APMs.
VISAPP 2025 - 20th International Conference on Computer Vision Theory and Applications
828

Our findings show that by leveraging video-based
analysis and state-of-the-art object tracking tech-
niques, we were able to generate detailed perfor-
mance metrics such as path length, velocity, accelera-
tion, jerk, and working area. These metrics may offer
an objective and data-driven approach to evaluate sur-
gical performance.
While we can successfully extract the aforemen-
tioned APMs from input videos, we are currently not
able to evaluate how these APMs translate to surgical
performance. Making such an evaluation would re-
quire thorough analysis of the videos by one or more
expertly trained surgeons. This analysis could poten-
tially be correlated with the extracted APMs to de-
termine what classifies as good surgical performance.
Thus, given the APMs of the videos, we can only
compare the scores between different videos. Future
work is required to determine how well the extracted
APMs can predict surgical performance.
Moreover, it is not currently possible for us to
evaluate the accuracy of the APMs we have calcu-
lated. The datasets we have acquired do not include
ground truth data regarding the positioning of the
tools relative to the environment they are in. Be-
cause of this, we cannot make conclusions about how
good our APM estimates are, but only conclude about
comparison between one video’s surgery performance
over another. One factor that could also potentially in-
troduce error is the spatial component in some APMs,
such as velocity, acceleration, jerk, and path length,
because the calculation requires depth information.
The tools move around in all directions, making it
hard to estimate depth from 2D videos. It might be
possible to estimate this if the camera parameters are
known, but these parameters are not available for the
datasets that we have used.
Additionally, the nature of laparoscopic surgeries
introduces further complexity. These surgeries of-
ten involve a person manually holding the camera,
leading to slight movements that can add noise to
the APM calculations. This camera movement is not
taken into account when calculating the APMs.
Although APMs are still in their infancy, this
emerging field holds significant promise for trans-
forming surgical training and enhancing the perfor-
mance of experienced surgeons. APMs can provide
actionable feedback to surgeons, potentially reducing
the reliance on high surgical volumes for skill acqui-
sition. With the current constraints on surgical care
limiting procedure volumes, the development and re-
finement of APMs offer a viable solution to optimize
training and performance evaluation. Future research
should focus on expanding the repertoire of APMs
and advancing their accuracy and applicability in as-
sessing surgical performance.
6 CONCLUSION
In this project, we developed an automated system
to evaluate surgical performance, providing a foun-
dation for improved assessment methods. The pri-
mary objective was to create a pipeline capable of
processing laparoscopic surgery videos, detecting and
tracking surgical instruments, and calculating APMs
to support objective evaluation.
The fine-tuned YOLO11 model demonstrated
strong performance on the m2cai16-tool-locations
dataset, achieving a mean average precision
(mAP@0.5) of 0.957. However, on the Cholec80-
Boxes dataset, it scored a lower mAP@0.5 of 0.65,
highlighting dataset-dependent variability. Despite
this, the model provided a robust foundation for
tracking.
For tracking, ByteTrack, BoT-SORT, and Uni-
Track were evaluated using established MOT metrics
such as HOTA, MOTA, and IDF1. These MOT met-
rics helped identify BoT-SORT as the most effective
tracker for this application, balancing detection ac-
curacy and identity association across the evaluation
metrics.
The system successfully extracted APMs, such
as path length, velocity, acceleration, jerk, working
area, and usage time distribution, enabling compara-
tive analyses between surgical videos. Future work
should address our limitations to improve APM accu-
racy.
In conclusion, this work validates state-of-the-art
detection and tracking algorithms’ ability to compute
APMs from 2D laparoscopic surgery videos. This
project lays a foundation to improve the quality and
fidelity of surgical training, offering a potential in en-
hancing patient safety and reducing training costs.
ACKNOWLEDGMENT
We would like to thank Aalborg University for pro-
viding the computational resources needed for this
project.
REFERENCES
Abdulbaki Alshirbaji, T. et al. (Aug. 2024). Cholec80-
Boxes: Bounding-Box Labels for Surgical Tools in
Five Cholecystectomy Videos. Zenodo. DOI: 10 . 5281/
Automated Performance Metrics for Objective Surgical Skill Assessment in Laparoscopic Training
829

zenodo . 13170928. URL: https : / / doi . org / 10 . 5281 /
zenodo.13170928.
Aharon, N., R. Orfaig, and B.-Z. Bobrovsky (2022). “BoT-
SORT: Robust Associations Multi-Pedestrian Track-
ing”. In: arXiv preprint arXiv:2206.14651.
Benchmark", " O. T. (n.d.). Accessed on: Dec. 11, 2024.
[Online]. Available: https://www.MOTChallenge.net.
Buckley, C. E. et al. (2015). “Zone calculation as a tool for
assessing performance outcome in laparoscopic sutur-
ing”. In: Surgical Endoscopy 29, pp. 1553–1559.
Chen, J. et al. (2018). “Use of automated performance met-
rics to measure surgeon performance during robotic
vesicourethral anastomosis and methodical develop-
ment of a training tutorial”. In: The Journal of urology
200.4, pp. 895–902.
Code", " with (n.d.). Accessed on: Dec. 11, 2024 [Online].
Available: https://www.paperswithcode.com.
D’Angelo, A.-L. et al. (2015). “Idle time: an underdevel-
oped performance metric for assessing surgical skill.”
In: American journal of surgery 209, pp. 645–651.
Ebina, K. et al. (2022a). “Automatic assessment of laparo-
scopic surgical skill competence based on motion met-
rics”. In: PLoS one 17.11, e0277105.
— (2022b). “Objective evaluation of laparoscopic surgi-
cal skills in wet lab training based on motion analy-
sis and machine learning”. In: Langenbeck’s archives
of surgery 407.5, pp. 2123–2132.
Guerin, S. et al. (2022). “Review of automated performance
metrics to assess surgical technical skills in robot-
assisted laparoscopy”. In: Surgical Endoscopy, pp. 1–
18.
J Luiten. A Ošep., P. D. e. a. (2021). “HOTA: A Higher
Order Metric for Evaluating Multi-object Tracking”. In:
International Journal of Computer Vision 129, pp. 548–
578. URL: https://doi.org/10.1007/s11263-020-01375-
2.
Jin, A. et al. (2018). Tool Detection and Operative Skill
Assessment in Surgical Videos Using Region-Based
Convolutional Neural Networks. arXiv: 1802 . 08774
[cs.CV]. URL: https://arxiv.org/abs/1802.08774.
Jocher, G. and J. Qiu (2024). Ultralytics YOLO11. Ver-
sion 11.0.0. URL: https : / / github . com / ultralytics /
ultralytics.
Moglia, A. et al. (2021). “A systematic review on artificial
intelligence in robot-assisted surgery”. In: International
Journal of Surgery 95, p. 106151.
Peng, W. et al. (2019). “An automatic skill evaluation
framework for robotic surgery training”. In: The Inter-
national Journal of Medical Robotics and Computer
Assisted Surgery 15.1, e1964.
Reiley, C. E. et al. (2011). “Review of methods for objec-
tive surgical skill evaluation”. In: Surgical endoscopy
25, pp. 356–366.
Rivas-Blanco, I. et al. (2021). “A review on deep learn-
ing in minimally invasive surgery”. In: IEEE Access 9,
pp. 48658–48678.
Sallaberry, L. H., R. Tori, and F. L. Nunes (2022). “Au-
tomatic performance assessment in three-dimensional
interactive haptic medical simulators: A systematic re-
view”. In: ACM Computing Surveys 55.7, pp. 1–35.
Schmidt, A. et al. (2024). “Tracking and mapping in med-
ical computer vision: A review”. In: Medical Image
Analysis 94, p. 103131. ISSN: 1361-8415. DOI: https :
/ / doi . org / 10 . 1016 / j . media . 2024 . 103131. URL:
https : / / www. sciencedirect . com / science / article / pii /
S1361841524000562.
Trejos, A. L. et al. (2014). “Development of force-based
metrics for skills assessment in minimally invasive
surgery”. In: Surgical endoscopy 28, pp. 2106–2119.
Twinanda, A. et al. (Feb. 2016). “EndoNet: A Deep Archi-
tecture for Recognition Tasks on Laparoscopic Videos”.
In: IEEE Transactions on Medical Imaging 36. DOI: 10.
1109/TMI.2016.2593957.
Wang, Z. et al. (2021). “Do different tracking tasks require
different appearance models?” In: Advances in Neural
Information Processing Systems 34, pp. 726–738.
Zhang, Y. et al. (2022). “ByteTrack: Multi-Object Tracking
by Associating Every Detection Box”. In.
VISAPP 2025 - 20th International Conference on Computer Vision Theory and Applications
830
