
From Interpretability to Clinically Relevant Linguistic Explanations:
The Case of Spinal Surgery Decision-Support
Alexander Berman
1 a
, Eleni Gregoromichelaki
1 b
and Catharina Parai
2,3 c
1
Centre for Linguistic Theory and Studies in Probability, Dept. of Philosophy, Linguistics and Theory of Science, University
of Gothenburg, Sweden
2
Department of Orthopedics, Sahlgrenska University Hospital, Gothenburg, Sweden
3
Sahlgrenska Academy, University of Gothenburg, Sweden
{alexander.berman, eleni.gregoromichelaki}@gu.se, catharina.parai@vgregion.se
Keywords:
Interpretable AI, Machine Learning, Explanations, Linguistics, Argumentation Theory, Decision-Support
Systems, Spinal Surgery.
Abstract:
Interpretable models are advantageous when compared to black-box models in the sense that their predictions
can be explained in ways that are faithful to the actual reasoning steps performed by the model. However,
interpretability does not automatically make AI systems aligned with how explanations are typically com-
municated in human language. This paper explores the relationship between interpretability and linguistic
explanation needs of human users for a particular class of interpretable AI, namely generalized linear models
(GLMs). First, a linguistic corpus study of patient-doctor dialogues is performed, resulting in insights that can
inform the design of clinically relevant explanations of model predictions. A method for generating natural-
language explanations for GLM predictions in the context of spinal surgery decision-support is then proposed,
informed by the results of the corpus analysis. Findings from evaluating the proposed approach through a
design workshop with orthopaedic surgeons are also presented.
1 INTRODUCTION
In research concerning how to explain outputs from
AI systems, two main paradigms have evolved. Post-
hoc explanations methods such as LIME (Ribeiro
et al., 2016) and SHAP (Lundberg and Lee, 2017)
give some insight into how deep neural networks and
other black-box models make their inferences. In con-
trast, predictions from interpretable models (or so-
called “glass-box AI”) operate according to reasoning
steps that are, at least in principle, comprehensible for
humans (Rudin, 2019; Rudin et al., 2022).
Is is sometimes argued that interpretable models
are superior to black-box models in the sense that pre-
dictions can be explained in ways that are inherently
faithful to the actual reasoning steps executed by the
model, making interpretable models more adequate
in high-stakes applications (Rudin, 2019). Neverthe-
less, research concerning interpretable models largely
focuses on efforts to develop well-performing mod-
a
https://orcid.org/0000-0003-0513-4107
b
https://orcid.org/0000-0002-6933-5314
c
https://orcid.org/0000-0002-8332-0426
els (see, e.g. (Rudin et al., 2022)), leaving the re-
lationship between interpretability and users’ expla-
nation needs in AI-assisted decision-making largely
unexplored. This gap in previous research concerns
both how model interpretability can be leveraged to
obtain linguistic explanations that meet users’ needs,
and how such fulfilment of such needs depends on
formal properties of interpretable models (sparsity,
monotonicity, etc.).
This paper takes a step towards bridging this gap.
Specifically, the paper focuses on a particular class
of interpretable AI, namely generalized linear mod-
els (GLMs), in the context of spinal surgery decision-
support. As its main contribution, the paper pro-
poses a method for generating concise and clinically
relevant linguistic explanations for predictions from
GLMs, informed by communicative strategies ob-
served in doctor-patient conversations.
The proposed method is applied in the context of
a web-based instrument used by spine clinics in Swe-
den. The purpose of the instrument is to assist doctors
and patients during medical consultations where de-
cisions concerning choice of treatment (usually sur-
gical or non-surgical treatment) are made. Based
Berman, A., Gregoromichelaki, E. and Parai, C.
From Interpretability to Clinically Relevant Linguistic Explanations: The Case of Spinal Surger y Decision-Support.
DOI: 10.5220/0013403800003890
Paper published under CC license (CC BY-NC-ND 4.0)
In Proceedings of the 17th International Conference on Agents and Artificial Intelligence (ICAART 2025) - Volume 1, pages 909-920
ISBN: 978-989-758-737-5; ISSN: 2184-433X
Proceedings Copyright © 2025 by SCITEPRESS – Science and Technology Publications, Lda.
909

on GLMs, the tool predicts two patient-reported out-
comes of hypothetical surgery, as well as length of in-
hospital stay, for patients with degenerative spinal dis-
orders. The present study explores how the currently
deployed instrument, which does not offer patient-
specific explanations, can be modified and extended
to meet doctors’ and patients’ clinical needs related
to explainability.
The rest of the paper is organized as follows. Sec-
tion 2 situates the work in relation to previous ap-
proaches to generating linguistic explanations for in-
terpretable models. Section 3 is devoted to a lin-
guistic corpus study, where explanations for medi-
cal judgements are collected from existing corpora
and analysed in terms of communicative explanatory
strategies. Implications of the analysis for the de-
sign of clinically relevant linguistic explanations are
also discussed. In Section 4, a method for generat-
ing linguistic explanations of predictions from GLMs
is proposed, informed by the findings from the cor-
pus study. The section presents technical details con-
cerning the proposed method, as well as a preliminary
evaluation of the proposed method through a design
workshop with orthopaedic surgeons. Finally, Section
5 offers conclusions and discusses future work.
2 RELATED WORK
The perhaps earliest example of natural-language
explanations in the context of interpretable AI is
SHRDLU (Winograd, 1971), a system which can ex-
plain its rule-based reasoning. For example, when the
user asks why the system picked up a certain object,
it may respond: “To get rid of it”; when asked why
it got rid of it, it may respond: “To clean off the red
cube”, etc. In a similar vein, the more recent sys-
tem DAISY (Wahde and Virgolin, 2023) can (exhaus-
tively) explain how its use of hand-crafted or interac-
tively learned procedures yields specific results. For
example, when explaining how it concluded that the
largest city in France is Paris, it states: “I retrieved all
items in the city category”, “Then I found all items
belonging to France”, etc. Methods for producing
enthymematic (logically incomplete) explanations for
answers inferred on the basis of facts and rules are
proposed by (Xydis et al., 2020; Breitholtz, 2020;
Maraev et al., 2021). For example, if the user asks
why the system described by (Maraev et al., 2021)
recommends a particular route, it responds: “Because
the route is the shortest”, thereby stating a fact whose
relevance with respect to the explanandum hinges on
the implicit premise that short routes are better than
long ones. In contrast to these approaches, this paper
targets explanations for predictions from statistical
models. Various such approaches have been proposed
for black-box models, based on post-hoc explanation
techniques (see, e.g. (Forrest et al., 2018; Kaczmarek-
Majer et al., 2022; Slack et al., 2023)). One popular
explanation strategy is to rank the most important fea-
tures. For example, the system presented by (Slack
et al., 2023) generates explanations on the form ”For
[this prediction], the importance of the features have
the following ranking, where 1 is the most important
feature: 1: glucose, 2: bmi, 3: age ...” Presumably,
the lack of easily identifiable warrants makes such
explanations difficult to understand, or cause a false
sense of understanding when explainees identify war-
rants that do not reflect the actual inner workings of
the model (Berman, 2024b).
Post-hoc explanation methods can also be used
for interpretable models, by treating them as black
boxes (see, e.g. (Ahmed et al., 2024)). As for ap-
proaches that instead leverage interpretability, (Baaj,
2022) shows how explanations can be generated for
possibilistic and fuzzy rule-based systems. For exam-
ple, a justification for the judgement that a patient’s
blood sugar level will not be low can be generated
as: “This is mainly due to the fact that it is quite
certain that the activity consists of drinking coffee,
lunch or dinner and that the current blood sugar level
is medium or high.” A method for explaining predic-
tions by decision trees and fuzzy rules is presented by
(Alonso and Bugar
´
ın, 2019), enabling explanations
such as “Beer is type Porter because its strength is
standard and its color is brown”.
The method presented in this paper builds on work
by (Berman, 2024a), who proposes an interactive
method for generating explanations for predictions by
linear additive models, based on Toulmin’s theory of
argumentation (Toulmin, 2003). The method sup-
ports generation of both “data” (case-specific facts)
and “warrants” (general statistical patterns). For ex-
ample, if the model predicts that a person is intro-
verted (based on her music preferences), the most im-
portant datum can be expressed as “The person likes
high-energy music”, with the corresponding warrant
“Statistically, people that like high-energy music are
more likely to be introverted.” As detailed in Sec-
tion 4, the present work extends this approach to han-
dle a broader range of feature types (rather than only
continuous features). Furthermore, the present paper
shows how feature encoding can be jointly optimized
for performance and linguistic intelligibility.
Almost none of the previous approaches have
been empirically validated with end users. The only
exception is (Slack et al., 2023) who let participants
solve explainability-related tasks using two different
IAI 2025 - Special Session on Interpretable Artificial Intelligence Through Glass-Box Models
910

tools. However, the purpose of this validation was
to compare the authors’ conversational tool with a
graphical interface; the extent to which the tasks or
generated explanations were deemed clinically rele-
vant by participants was not studied.
In contrast to previous approaches, the present
work grounds the proposed natural-language genera-
tion method in a linguistic analysis of human explana-
tory interaction, and evaluates the method with end
users in a clinically relevant scenario.
3 LINGUISTIC CORPUS STUDY
To inform the design of linguistic explanations, a
qualitative linguistic corpus study is conducted by
collecting and analysing examples of how doctors
and patients explain (or support, or argue for/against)
judgements (e.g. certain treatments) in clinical set-
tings. Two empirical sources of clinical dialogues
were chosen: the Norwegian Corpus of Doctor-
Patient Consultations from Ahus (Gulbrandsen et al.,
2013) (henceforth abbreviated Ahus), and a Swedish
textbook in medicine focusing on the encounter be-
tween patient and doctor (Lindgren and Aspegren,
2004) (henceforth abbreviated L&A). The choice of
empirical material is primarily motivated by the topics
and types of situations that it encompasses. Further-
more, while one of the corpora (Ahus) is descriptive
and contains transcripts of actual consultations, the
other (L&A) is prescriptive and conveys communica-
tive norms. Both types of linguistic data were deemed
relevant for the purposes of the research.
The linguistic analysis builds on Toulmin’s the-
ory of argumentation (Toulmin, 2003). Toulmin iden-
tifies elements of arguments, including the claim
(corresponding to the explanandum), data (specific
facts that support the claim), and warrants (general
norms or rules of thumb that justify how facts support
claims). For example, the claim “you have a cold”
can be supported (explained) by the datum “you have
a runny nose”, which in turn rests on warrants such as
“runny nose is a symptom of a common cold”.
Specifically, the corpus study aims to answer the
following research questions:
1. To what extent do interlocutors (doctors and pa-
tients) explicitly convey argumentative elements
(claims, data, and warrants)?
2. To what extent do interlocutors implicitly convey
argumentative elements?
3. How do interlocutors linguistically indicate the re-
lationship between argumentative elements?
The RQs were purposely formulated in relation to the
intended downstream application of the results, i.e.,
design of linguistic explanations of predictive mod-
els. Specifically, claims are conceived to be poten-
tially analogous with statistical predictions, data with
feature values, and warrants with statistical patterns
learned by predictive models. In other words, it is
assumed in principle conceivable that doctors reason
in ways that are analogous (to some extent) with how
machine-learning models make predictions.
3.1 Corpus Data
Occurrences of explanations (or related phenomena
such as arguments or justifications) pertaining to med-
ical judgements were identified using a search proce-
dure. In the case of Ahus, which contains transcrip-
tions of 220 consultations, this was done by search-
ing for the word “why” (“hvorfor” in Norwegian); for
L&A, the corpus was small enough to permit a man-
ual search of the entire empirical material.
The topic of interest (medical judgements) pri-
marily encompasses diagnosis (judging that a patient
has a certain condition) and recommendations (judg-
ing that a particular action or intervention is ade-
quate). The selection procedure resulted in two dia-
logues from each corpus, spanning a total of 88 utter-
ances.
3.2 Annotation
To address the RQs, the data was annotated with the
following labels (hypothetical examples in parenthe-
ses):
• claim (“I think that you have a cold”)
• datum (“since you have a runny nose”)
• warrant (“since runny nose is a symptom of a com-
mon cold”)
Note that arguments are not assumed a priori to
be marked with particular syntactic constructions or
particles such as “since”, “because”, or “therefore”
(Sbis
`
a, 1987).
A complete annotation was first done by one of
the authors (with expertise in cognitive science, lin-
guistics, and machine learning), and then reviewed by
the two other authors (with expertise in linguistics and
medicine respectively). During the reviews, annota-
tions were open for collaborative amendments.
3.3 Analysis
The analysis reveals that in the empirical material,
claims are explicitly supported by up to three pieces
From Interpretability to Clinically Relevant Linguistic Explanations: The Case of Spinal Surgery Decision-Support
911

of data, whereas warrants are rarely communicated
explicitly. For example, in one of the dialogues, the
doctor expresses an intent to have the patient’s lungs
x-rayed (claim), which is justified with reference to
the patient’s low levels of oxygen in the blood (da-
tum). There is no explicit mention of how a person’s
levels of oxygen explain the recommendation to per-
form lung x-ray (warrant).
In cases where warrants are made explicit, they are
sometimes causal in nature. For example, in one di-
alogue, the patient expresses a wish to have her heart
checked-up since she gets very dizzy and wonders if
this is due to low blood pressure. In response, the doc-
tor explains that the patient’s dizziness can be caused
by her diabetes. However, in many cases, arguments
seem compatible with either causal or statistical war-
rants. For example, when a doctor judges that the
patient has no respiratory illness partly on the basis
that the “chest X-ray was completely normal”
1
, this
is compatible with either a causal warrant (e.g. res-
piratory illnesses cause abnormalities that can be de-
tected in a chest X-ray) or a statistical one (e.g. a nor-
mal chest X-ray correlates with absence of respiratory
illness).
Although warrants are rarely verbalized, data are
very frequently conveyed in ways that indicate what
kind of warrant the speaker might have in mind. In
one excerpt, the doctor says that the patient’s oxygen
levels are “a bit lower than one would expect”. Al-
though no warrant is explicitly conveyed, the words
“lower” and “expect” both allude at a warrant such as
“unexpectedly low levels of oxygen in the blood can
indicate lung disease”. In another example, the doctor
explains a recommended change of medication as fol-
lows: “since you have had [the medication for] over
two months and have increased the dosage and not
had any effect”; here, the lexical choices “over”, “in-
creased”, and “not ... any” trigger a warrant such as
“having used a medication for a long time without any
effects motivates trying another medication”.
Generally, two types of warrant triggers can
be observed in the data: scalar/gradable and
norm/expectation related. Examples of scalar trig-
gers include lower (levels of oxygen in the blood than
one would expect), over (two months of medication
use), increased (dosage), and no (effect of medica-
tion). Examples of norm-related warrant triggers in-
clude expected (levels of oxygen in the blood), nor-
mal (lung x-ray), abnormal (nothing abnormal in pa-
tient’s lungs), should (nothing observed that shouldn’t
be there), and good (cholesterol levels).
Although linguistic triggers help explainees to
1
Cited excerpts from the empirical material have been
translated to English by the authors.
identify potentially relevant warrants, a certain
amount of argumentative underspecification (ambigu-
ity) can be observed. For example, conveying oxygen
level in the blood as lower than expected is compat-
ible with a warrant that posits a monotonically de-
creasing relation between oxygen level in the blood
and the risk of lung disease. However, it is also
compatible with a non-monotonic relationship, i.e.
that too high oxygen levels in the blood also indi-
cate a higher risk of disease. Similarly, when mul-
tiple pieces of data are presented in support of a claim
(such as having used a medication for a long time with
a high dosage), potential interactions between data re-
main unstated. This kind of underspecification can
potentially be understood as serving the purposes of
relevance and brevity, i.e. only presenting informa-
tion that is deemed relevant for the patient, and not
providing more information than needed in the con-
text (cf. Grice’s maxims of relation/relevance and
quantity (Grice, 1975)).
As an additional finding, we observe that in-
terlocutors sometimes discuss mutually opposing
claims. For example, in one dialogue, the patient ex-
presses a wish to have her heart checked-up, while
the doctor argues that the patient’s dizziness can be
caused by her diabetes and that her blood pressure is
fine, thereby constructing a counter-claim that a heart
check-up is not needed.
3.4 Implications for Linguistic Design
of Model Explanations
When using the results of the corpus study to in-
form the design of clinically relevant explanations for
model predictions, several guiding principles can be
distilled. First, given the limited amount of conveyed
data per claim in human-human dialogues, it is ad-
visable to focus specific (local) explanations only on
those features that are most important to the predicted
outcome.
Second, given the consistent use of warrant trig-
gers in the presentation of data, and the explanatory
function that these triggers can be assumed to carry,
it is advisable to formulate data in ways that allude to
the corresponding statistical patterns learned by the
model. For scalar triggers, this can be done by choos-
ing a suitable modifier. For example, if the model
has learned that older age is associated with a lower
probability of being satisfied with surgery, and the pa-
tient’s age is statistically low, the patient’s age can be
presented as “relatively young”. Norm/expectation
triggers can also be conceived, e.g. “unexpectedly
high pain levels in the arm”. However, in the present
clinical context, this was not deemed applicable.
IAI 2025 - Special Session on Interpretable Artificial Intelligence Through Glass-Box Models
912

Third, given that interlocutors sometimes ex-
change claims and counter-claims, and give reasons
both for and against judgements, it is advisable to
convey circumstances that both support and contra-
dict a certain prediction (cf. (Miller, 2023)).
Furthermore, to provide more detailed informa-
tion about the statistical patterns learned by the model
and thereby help resolve potential ambiguities, ex-
plicit warrants could be offered. However, given that,
in the studied corpora, warrants were primarily con-
veyed implicitly, warrants should only be presented
on demand.
Finally, it is worth noting that the observed usage
of causal warrants in human-human dialogues may in-
dicate that statistical explanations may not always be
satisfactory or sufficient for users (as previously ar-
gued by e.g. (Miller, 2019)). For example, a corre-
lation between low disability and high probability of
successful surgery might be difficult to comprehend
without resorting to causal reasoning of some kind
(such as disability causing depression or other psy-
chological states that in turn influence pain percep-
tion). In principle, generated explanations for model
predictions could include such causal links, poten-
tially collected from domain experts and built into
the tool. However, such explanations could invite
false inferences concerning how the model actually
reasons. For this reason, we argue that generated
warrants should only convey actual statistical patterns
learned by the model, leaving causal matters open for
interpretation.
4 GENERATING CLINICALLY
RELEVANT EXPLANATIONS
Swedish spine clinics have access to an AI-based
“Dialogue Support” tool whose purpose is to assist
patients and doctors in their decision-making con-
cerning treatment options for four different types of
degenerative spinal disorders: disc herniation and
spinal stenosis in the lumbar spine respectively, or
chronic low back pain, as well as cervical radiculopa-
thy (Fritzell et al., 2022). The tool is used by the
doctor and patient together during brief (approx. 20
minutes) medical consultations. Based on sociode-
mographic information (age, gender, etc.) and other
answers provided by the patient in a questionnaire, the
tool presents predictions for three types of outcomes
of a hypothetical surgery:
• Satisfaction: the probability of responding to the
question “What is your attitude towards the result
of the surgery?” with one of the first two options
in the Likert scale satisfied, hesitant, dissatisfied
one year after surgery.
• Global Assessment (GA): the probability of re-
sponding to the question “How is your pain to-
day as compared to before the surgery?” with one
of the first two options in the Likert scale com-
pletely pain-free, much better, somewhat better,
unchanged, worse one year after surgery.
• Length of stay: the number of days of hospital-
ization in connection with the surgery.
The predictions are based on three different types of
GLMs trained on patient data from the national qual-
ity registry Swespine. Currently, the Dialogue Sup-
port tool explains its predictions “globally”, with in-
formation about features, sample size, etc. No case-
specific (“local”) explanations are presented.
In the subsequent sections, a method for gen-
erating linguistic explanations for predictions from
GLMs will be proposed, with the purpose of enabling
an alternative Dialogue Support tool based on the
same patient data and types of models. The proposed
method builds on previous work by (Berman, 2024a),
which is extended to support needs and desiderata
identified in the corpus study, as well as feedback
collected in a design workshop with orthopaedic sur-
geons (see Section 4.7).
2
4.1 Model Specification
GLMs estimate an outcome on the basis of a lin-
ear combination of predictors (independent variables)
and a link function that transforms the linear combi-
nation to an outcome:
E[Y | X ] = g
−1
β
0
+
∑
i
X
i
β
i
!
where E[Y | X] is the expected value of the outcome
Y given the intercept (bias) term β
0
, the predictors
X
i
, the coefficients β
i
, and the link function g. For
the purposes at hand, g is assumed to be monotonic,
which is typically the case. Specifically, in the study
at hand, g is either
• logit (i.e. logistic regression), for estimating sat-
isfaction,
• threshold function for the cumulative distribution
function (i.e. ordered probit), for estimating GA,
or
• rounding to non-negative integer (linear (Ridge)
regression adapted to counts), for predicting
length of stay.
2
While the prototype currently supports Swedish, this
paper uses English translations.
From Interpretability to Clinically Relevant Linguistic Explanations: The Case of Spinal Surgery Decision-Support
913

One model is used for each combination of diagnosis
and task (type of outcome). Since there are 4 diag-
noses and 3 tasks, a total of 12 models is used.
4.2 Datasets
Historical patient data was obtained from the Swe-
spine registry in the form of one dataset per diagno-
sis. The 4 datasets together encompass 37 features.
Table 1 presents the feature types, with examples of
features.
For the purposes of the study, features were se-
lected to jointly optimize for performance and spar-
sity. This was done using backward elimination, with
area under the ROC curve (AUC) as performance
metric for satisfaction and GA, and mean absolute
error (MAE) for length of stay. Among the best-
performing feature sets (i.e. performance not worse
than the best performance minus a tolerance thresh-
old), the feature set with the smallest number of fea-
tures was selected.
4.3 Feature Encoding
Different feature types/encodings afford distinct lin-
guistic expressions of data and warrants. Numeric
features enable the use of scalar triggers such as
“young age” or “no pain in the back”. For example,
if the patient’s young age is presented as a positive
factor, this invites the inference that the model gen-
erally associates a lower age with a more favourable
outcome.
Binary features enable self-evident warrant-
triggering contrasts. For example, if the patient being
female is presented as a positive factor, this implies
that female patients are generally estimated to have a
more favourable outcome than male patients.
In the case of multinomial categorical features,
warrants are not as straightforwardly triggered. For
example, if the fact that the patient is “treated at a uni-
versity clinic” (rather than a public or private clinic) is
presented as indicative of a negative outcome, a corre-
sponding warrant cannot easily be identified. Specif-
ically, the formulation does not convey whether the
prediction would be more positive if treated in a pub-
lic or private clinic. Since not many multinomial cat-
egoricals were among the most predictive features in
the studied case, this problem was not addressed.
As for ordinals, the picture is more nuanced. At
least two approaches can be conceived: to treat them
either as numeric or as multinomial categorical fea-
tures. In line with the reasoning above, numeric en-
coding is more favourable from the perspective of
linguistic intelligibility. However, a categorical en-
coding may yield better performance. To this end,
the choice of encoding for ordinals was made in a
flexible way. Specifically, high-cardinality ordinals
(> 5 values) were encoded numerically, since it was
deemed highly unintuitive to treat each value on a
10-item pain scale as its own category. As for low-
cardinality ordinals, a data-driven approach was em-
ployed to jointly optimize for linguistic intelligibility
and performance. Among the best-performing encod-
ing candidates (i.e. performance not worse than the
best performance minus a tolerance threshold), the
feature set with the largest amount of numeric encod-
ings was selected.
3
The proposed strategy for choosing feature encod-
ings is summarized in Table 1.
4.4 Interface Design
Local explanations are presented in a waterfall chart,
where the estimated outcome is visualized in terms
of the outcome for an average patient, and the cu-
mulative effect of data (see Figure 1), grouped into
positive and negative, and ordered by decreasing im-
portance. For example, a moderate probability of a
successful outcome can be explained by the fact that
the patient has no other illnesses (positive factor) and
relatively severe back pain (negative factor). A max-
imum of three positive and negative factors respec-
tively is shown by default; additional data can be re-
vealed by clicking “Show more”.
Outcomes are visualized along a probability scale
(for satisfaction and GA) or integer scale (for length
of stay), while data (feature contributions) are visual-
ized without any explicit scale. In other words, math-
ematically, the waterfall chart informally conveys:
4
E[Y |
¯
X] +
∑
β
i
(X
i
−
¯
X
i
) ≈ E[Y |X]
Warrants conveying information about the statistical
patterns learned by the model, e.g. that lower disabil-
ity is associated with a higher estimated probability
of a successful outcome, are presented inside a wid-
get titled “More information”. The widget also con-
tains information about the sample size and training
data, which argumentatively can be said to back the
warrants. The content of the widget is collapsed by
default, but can be expanded as needed.
3
Predictive performance after interpretability optimiza-
tions was AUC 0.65-0.69 for satisfaction, AUC 0.62-0.69
for GA, and mean absolute error 0.27-1.06 for length of
stay.
4
A completely faithful visualization would need to ac-
count for non-linearity of the link function. This degree of
faithfulness was not deemed motivated for the purposes at
hand.
IAI 2025 - Special Session on Interpretable Artificial Intelligence Through Glass-Box Models
914
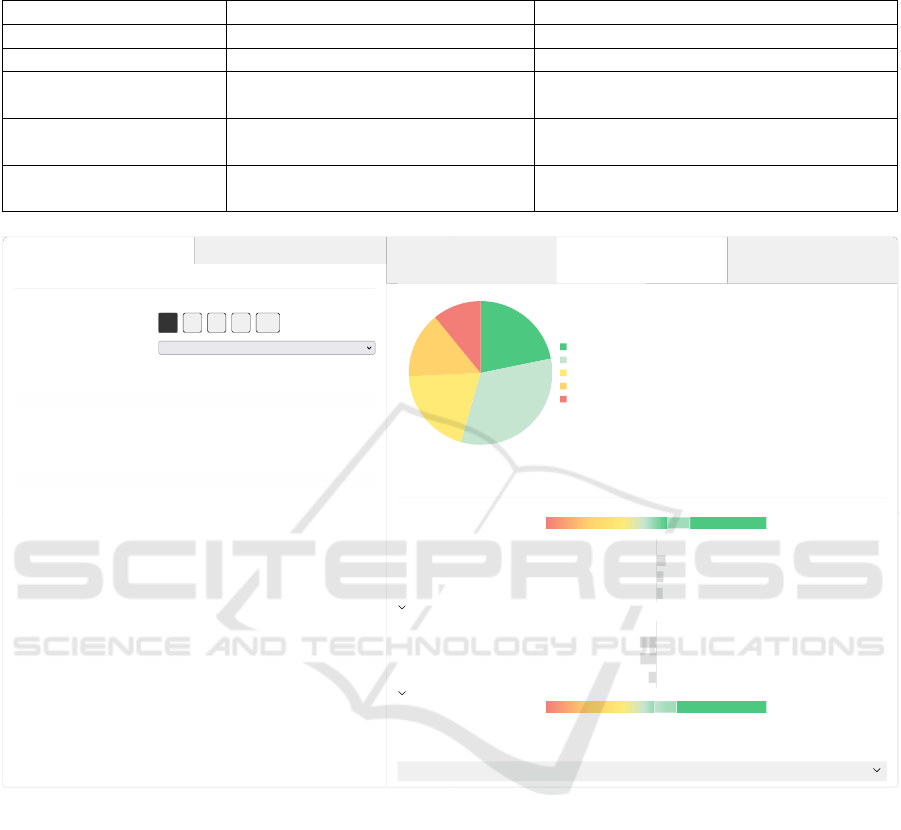
Table 1: Features types among the datasets used to train the predictive models. The reasoning behind the choice of encodings
is described in Section 4.3.
Feature type Encoding Example(s)
numeric standardization (continuous value) age, BMI
binary binary gender, employment status
multinomial categorical one-hot (dummy variables) clinic type (public, private, or university
hospital)
high-cardinality ordinal standardization (continuous value) pain levels (10-item scale from 0 (no pain)
to 10 (worst conceivable pain))
low-cardinality ordinal one-hot (dummy variables) or stan-
dardization (continuous value)
walking distance (5-item scale from 0-100
meters to more than 2 years)
Basic information
Back-specific information
Subgroup
Diagnosis Spinal stenosis
Operated levels 1 2 3 4 5+
Clinic type
University hospital
Height (cm) 168
Sociodemographics
Age 45
Unemployed No
Education level Primary/secondary level
Health profile
Previous spine surgery No
Comorbidity No
Probability of being satisfied
67%
Probability of successful outcome
55%
Expected length of stay
Approx. 2 days
The pie chart shows the probability of different pain levels after a hypothetical surgery, based on the chosen patient profile.
Explanation
Unsuccessful outcome Successful outcome
Average patient
Positive factors:
No previous spine surgery
Relatively low disability
No other illness
SHOW MORE
Negative factors:
Treated at university hospital
Relatively long duration of leg pain
Relatively long duration of back
pain
SHOW MORE
Combined probability
The pie chart shows how the probability of successful outcome of surgery (pain completeley gone or much improved after 1
year) is calculated based on the probability of successful outcome for an average patient and factors concerning the chosen
patient profile.
22%
33%
20%
15%
11%
Pain free
Much improved
Slightly improved
Unchanged
Worse
61%
55%
More information
Figure 1: Screenshot of the prototype, with a hypothetical patient profile.
4.5 Choice of Reference
As elaborated above, data are visually and linguis-
tically presented in relation to a reference. In the
proposed prototype, the reference is chosen as the
mean historical patient with the same diagnosis (R =
¯
X), although such a notion may be perceived as ab-
stract. The main reason for not settling with the in-
tercept/bias as reference is that this would introduce
an undesired bias for binary features; e.g. the gender
encoded as 0 (in this case being male) would never be
highlighted as a factor.
The frequently observed comparison with expec-
tation/norm in the corpus (see Section 3.3) may sug-
gest using “healthy patient” as a reference in medical
contexts where it can be clearly established a priori
what constitutes a “healthy” feature value. Allowing
reference to be chosen interactively may also be an
option.
4.6 Generation of Data and Warrants
The proposed method for generating linguistic ex-
planations for GLMs consists of general (domain-
and language-independent) functions for generating
data and warrants, which depend on a domain- and
language-specific grammar containing functions that
produce linguistic surface realizations. The overall
architecture of the proposed method is illustrated in
Figure 2.
From Interpretability to Clinically Relevant Linguistic Explanations: The Case of Spinal Surgery Decision-Support
915
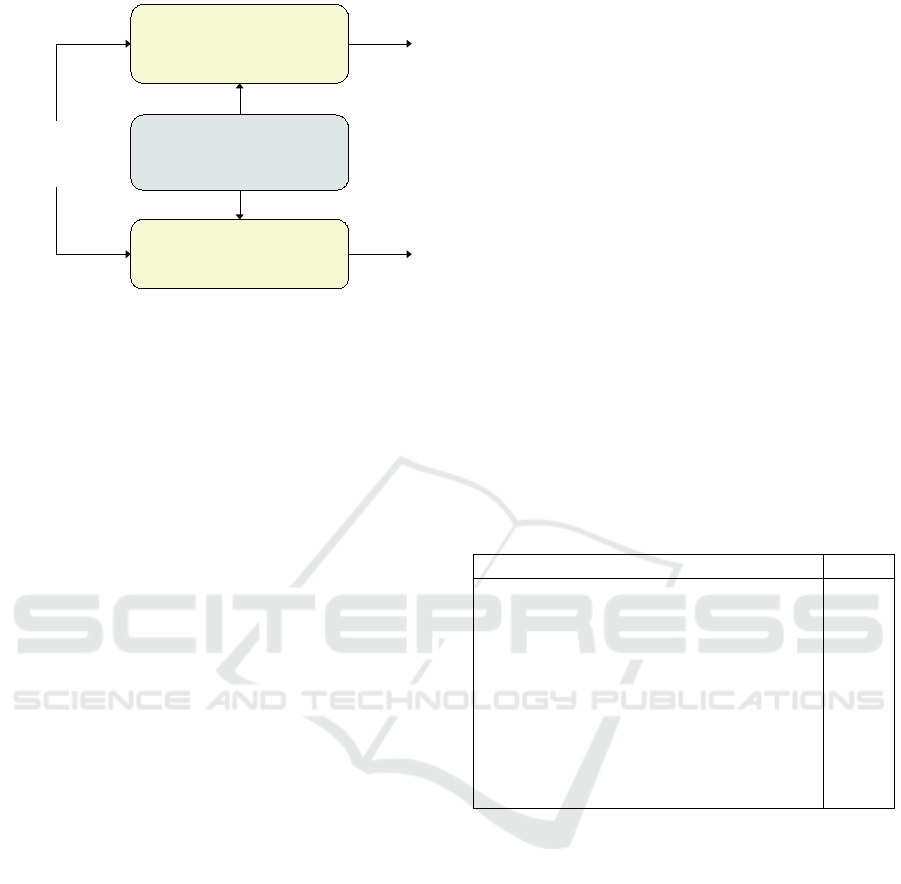
DATUM GENERATOR
Information
about feature
“Relatively mild back pain”
GRAMMAR
WARRANT
GENERATOR
“The less back pain, the higher the calculated probability of a
successful outcome. The difference can be up to 13 percentage points.”
Figure 2: Overall architecture of the proposed method for generating linguistic explanations for GLMs, with output examples
for the feature BackPain. Input to the datum and warrant generators consists of information such as feature type, feature
value, mean feature value, and coefficient.
4.6.1 Generation of Data
In the visualization of local explanations, data are ex-
pressed either with scalar triggers (e.g. “Relatively
young/old age”) or a bare linguistic label (e.g. “Fe-
male”), depending on the type of feature. Formally,
we define DatumPhrase(t, f , x, ¯x) as a general func-
tion that, given information about a feature, returns a
datum phrase. Specifically,
DatumPhrase(t, f , x, ¯x) =
(
FeatureLevelPhrase( f , Level(x, ¯x)) if t = numeric,
Label( f , x) if t = categor.
where f is the feature symbol, x = X
i
is the feature
value, and ¯x is the mean value of the feature for the
entire sample. FeatureLevelPhrase( f , l) is a gram-
mar function that generates a feature-level phrase for
feature f and level l (e.g. “Relatively young age” for
f = Age and l = low), while the grammar function
Label( f , x) returns a bare linguistic label (e.g. “Fe-
male” for f = Gender and x = 1). The general func-
tion Level(x, r) returns the level of the feature value x
in relation to a reference value r = R
i
. Specifically,
L(x, r) =
zero if x = 0,
low if 0 < x < r,
high x ≥ r
For the grammar functions FeatureLevelPhrase
and Label, the present work uses simple mappings
(see Figure 3).
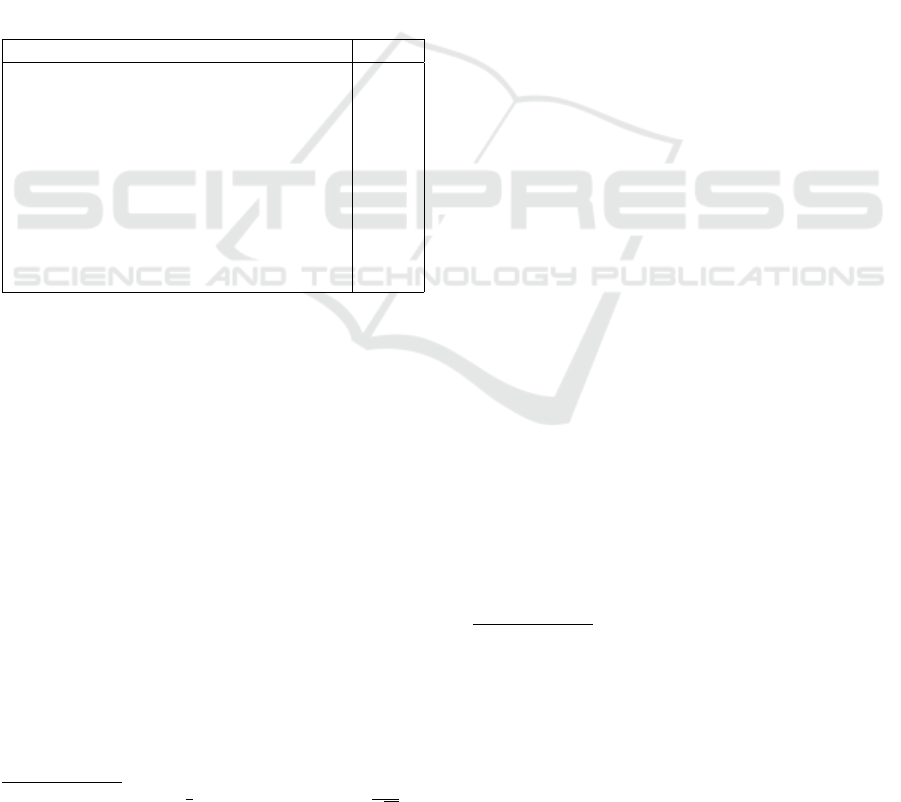
Results of applying the proposed method on his-
torical patients (i.e. instances in the datasets) are
shown in Table 2 and Table 3, presenting the 10 most
frequently occurring phrases for positive and negative
factors respectively.
Table 2: The 10 most frequently occurring phrases describ-
ing positive factors for historical patients, as generated by
the proposed method and aggregated across diagnoses and
outcomes. “Occurring” here means that the phrase is in-
cluded among the top three positive factors shown in the
interface. “Positive” refers to higher estimated probability
of satisfaction or successful outcome, or shorter duration of
stay. Frequencies are relative to the total number of patients.
Data presented as positive Freq.
Treated in private clinic 0.46
No other illnesses 0.35
No previous spine surgery 0.32
Relatively low disability 0.18
Relatively few operated levels 0.17
Relatively short duration of back pain 0.15
Has university education 0.13
Relatively mild back pain 0.13
Can walk relatively far in normal pace 0.12
No university education 0.12
Inferences that are invited by presenting data in
the manner described above are mathematically guar-
anteed to correctly reflect the actual reasoning steps
performed by the model. For example, if “relatively
mild back pain” (compared to an average patient)
is presented as a positive factor, this invites the in-
ferences that the patient has some amount of back
pain, but lower than an average patient, and that mild
back pain is associated with a more favourable pre-
dicted outcome than severe back pain. Mathemati-
cally, this corresponds to conveying X
i
<
¯
X
i
and that
β
i
(X
i
−
¯
X
i
) > 0 contributes positively to the outcome
(assuming a monotonically increasing inverse link
function), and linguistically inviting the factual infer-
ence 0 < X
i
<
¯
X
i
and the warrant inference β
i
< 0. The
correctness of the factual inference follows from the
condition for selecting the word “mild” (L(X
i
,
¯
X
i
) =
low iff 0 < X
i
<
¯
X
i
). As for the warrant inference,
IAI 2025 - Special Session on Interpretable Artificial Intelligence Through Glass-Box Models
916
FeatureLevelPhrase( f , l) =
if f = BackPain :
“No back pain” if l = zero,
“Relatively mild back pain” if l = low,
“Relatively severe back pain” if l = high
if f = . . .
Label( f , x) =
if f = Gender :
(
“Male” if x = 0,
“Female” if x = 1
if l = . . .
Figure 3: Examples of domain- and language-specific linguistic mappings belonging to an English grammar in the domain of
spinal disorders.
Table 3: The 10 most frequently occurring phrases describ-
ing negative factors for historical patients, as generated by
the proposed method and aggregated across diagnoses and
outcomes. “Occurring” here means that the phrase is in-
cluded among the top three negative factors shown in the
interface. “Negative” refers to lower estimated probability
of satisfaction or successful outcome, or longer duration of
stay. Frequencies are relative to the total number of patients.
Data presented as negative Freq.
Relatively high disability 0.19
Treated in public clinic 0.18
Relatively severe back pain 0.18
Has other illnesses 0.16
No university education 0.16
Relatively long duration of back pain 0.15
Relatively short height 0.13
Relatively many operated levels 0.13
Relatively old age 0.13
Relatively long duration of leg pain 0.10
its correctness can be verified as follows. Since
β
i
(X
i
−
¯
X
i
) > 0 and X
i
−
¯
X
i
< 0 (because X
i
<
¯
X
i
),
the product β
i
(X
i
−
¯
X
i
) can only be positive if β
i
< 0.
In other words, the mathematical guarantee hinges on
the monotonicity of the link function and on the linear
additive treatment of features.
4.6.2 Generation of Warrants
Warrants conveying correlations learned by the mod-
els are expressed in ways that communicate both ef-
fect size and, when relevant, polarity. For example,
the warrant for a numeric feature can be formulated
as: “The less back pain, the higher the calculated
probability of a successful outcome. The difference
can be up to 24 percentage points.” Effect sizes are
calculated with respect to the magnitude of the coeffi-
cient and the absolute maximum slope of the inverse
link function.
5
Table 4 shows generated warrants for a particular
5
|max((g
−1
)
′
(x))| is
1
4
for logistic regression,
1
√
2π
for
ordered probit, and 1 for linear regression.
diagnosis and outcome.
4.7 Evaluation
An early prototype of the proposed solution was eval-
uated through a design workshop with orthopaedic
surgeons. In the invitation, potential participants were
informed that they would test a new alternative inter-
face to the Dialogue Support tool, which they all had
experience of using. 3 out of 5 invited respondents
participated in the workshop on site, while one tested
the prototype individually and then gave written feed-
back via email.
6
In the first part of the workshop, participants indi-
vidually accessed the prototype, where a randomized
patient profile was shown.
7
They were then asked to
imagine having a dialogue with a patient who wants
to know why the computer estimates an X% probabil-
ity of successful outcome, and to answer the patient’s
question very briefly. Participants noted their answers
and were then asked to voluntarily read them aloud.
In the second part, participants were asked: “Is
there anything in the explanations that can be im-
proved?”
8
The discussion was moderated by the or-
ganizer of the workshop (one of the authors).
The version of the prototype tested by partici-
pants only supported one diagnosis (disc herniation)
and two outcomes (satisfaction and GA). Instruc-
tions were conveyed to participants verbally and via a
beamer presentation. Feedback was recorded in notes
and later organized according to themes.
6
One of the authors participated in the workshop in the
role of orthopaedic surgeon. This author had not been in-
volved in the development of the prototype or the organiza-
tion of the workshop.
7
The randomization was done individually for each par-
ticipant. Feature values were uniformly sampled from pre-
defined ranges.
8
Participants were also asked if there is anything else
with the alternative interface that can be improved. Results
from this part of the workshop are not reported here.
From Interpretability to Clinically Relevant Linguistic Explanations: The Case of Spinal Surgery Decision-Support
917

Table 4: Generated warrants conveying correlations for spinal stenosis and pain assessment (GA). Warrants are shown to users
when they click “More information” in the interface.
Disability The lower the disability, the higher the calculated probability of a successful outcome. The
difference can be up to 33 percentage points.
Leg pain du-
ration
The shorter the leg pain duration, the higher the calculated probability of a successful out-
come. The difference can be up to 19 percentage points.
Previous spine
surgery
Patients who have not undergone previous spine surgery are calculated to have a higher
probability of a successful outcome. The difference can be up to 14 percentage points.
Back pain The less back pain, the higher the calculated probability of a successful outcome. The
difference can be up to 13 percentage points.
Back pain du-
ration
The shorter the back pain duration, the higher the calculated probability of a successful
outcome. The difference can be up to 11 percentage points.
Comorbidity Patients with no other illnesses are calculated to have a higher probability of a successful
outcome. The difference can be up to 8 percentage points.
Unemployment Patients with employment are calculated to have a higher probability of a successful out-
come. The difference can be up to 8 percentage points.
Type of clinic Patients treated at private clinics are calculated to have the highest probability of a suc-
cessful outcome. Patients treated at university hospitals are calculated to have the lowest
probability of a successful outcome. The difference can be up to 7 percentage points.
4.7.1 Results
In the first part, one of the participants gave the fol-
lowing answer: “There is a 76% probability of be-
ing satisfied with surgery which is 10% worse than
an average pat[ient] who is operated for disc herni-
ation. The reason that it looks this way is that you
have had back pain for a longer time and furthermore
xxx diseases. Furthermore, your age gives you a sta-
tistically somewhat lower probability of a successful
result.” (our translation)
As for the second part, one participant com-
mented that the textual explanations for the model
and the specific outcomes were good and informa-
tive. Three suggestions related to global explanations
were raised. First, it was recommended to use pos-
itive instead of negative wording; e.g. substituting
expressions like “The older the age, the lower the...”
with “The younger the age, the higher the...”. Second,
the wording “is estimated” was advised to be replaced
with alternatives such as “is calculated,” “results have
previously shown,” or “based on previous patients’ re-
sults of surgery”. Third, it was suggested that features
should be sorted by descending effect size. All these
suggestions were subsequently accommodated.
A question was raised as to whether the correla-
tion between age and satisfaction is in reality “a curve
rather than linear”. The question highlights a discrep-
ancy between the participant’s domain knowledge and
monotonicity assumptions built into the model. The
fact that this discrepancy surfaced can be seen as a
positive finding, in the sense that the tool’s explana-
tion enabled the user to form a correct mental model
of how the AI reasons (and to contrast this model with
his/her own reasoning).
Two participants wondered if it would be adequate
to tell the patient that the model makes its prediction
based on data concerning other patients with similar
characteristics. In Toulmin’s framework, this relates
to backing, i.e. arguing for the general acceptability
of a warrant. To enable more accurate backing, infor-
mation was added in the tool to clarify that predictions
are made on the basis of the entire available sample of
patients with the diagnosis at hand.
One participant observed that some factors were
missing from the global explanations; this was later
attributed to a bug, which has since been resolved.
As an indirect finding, it was observed that no
questions or critical comments were raised regarding
the phrasing of data. Furthermore, when participants
exemplified how they would respond to the patient’s
request for an explanation, the participants seemed to
have interpreted the data as intended. This can be
taken as an indication that the generation of datum
phrases is serving its intended purpose.
In summary, the design workshop resulted in gen-
erally positive findings regarding the proposed lin-
guistic explanations, as well as suggested improve-
ments that have been accommodated into the proto-
type.
5 CONCLUSIONS AND FUTURE
WORK
Informed by a linguistic and argumentative analysis
of doctor-patient dialogues, this paper has proposed
IAI 2025 - Special Session on Interpretable Artificial Intelligence Through Glass-Box Models
918

a method for generating linguistic explanations for
predictions from GLMs in the context of a statisti-
cal instrument aiming to assist treatment decisions
concerning degenerative spinal disorders. Unlike
previous approaches to generating natural-language
explanations for predictions from statistical models,
the method proposed here is grounded in empirical
findings concerning analogous human communicative
strategies. Specifically, the proposed method linguis-
tically formulates salient case-specific facts in ways
that concisely indicate the underlying statistical pat-
terns used by the model, without overloading the user
with an exhaustive account of the model’s entire rea-
soning logic. This way, the approach balances pur-
poseful brevity with the possibility to get more de-
tailed information that reduces potential ambiguity re-
garding the model’s reasoning.
The simplicity of the concrete linguistic explana-
tions obtained with the proposed method (“relatively
young age”, etc.) reflects a desirable alignment with
how humans typically formulate explanations. No-
tably, this simplicity is not obtained at the cost of
reduced faithfulness, unlike with popular post-hoc
explanation methods for black-box models (such as
LIME and SHAP).
While the interface design and linguistic surface
realization presented in this paper are adapted to a
specific medical use case, the method as such is
simple in nature and straightforwardly generalizes to
other clinical use cases with similar needs, and po-
tentially also to other domains. Despite recent de-
velopments in deep neural networks and generative
AI, GLMs are still commonly used in high-stakes do-
mains such as healthcare, in part due to their inter-
pretability (Pantanowitz et al., 2024). From this per-
spective, one of the main implications of the pre-
sented work is to demonstrate how interpretability,
conceived as pertaining to certain abstract or for-
mal properties, can be leveraged in practice to obtain
downstream value in the form of linguistic explana-
tions that are aligned with how humans typically ex-
plain decisions and judgements. This can be poten-
tially valuable not only for AI-based decision support,
but also in situations where linguistically intelligible
explanations for AI-based decisions are required for
ethical or legal reasons (see, e.g. (Berman, 2024b)).
On a theoretical level, the work also shows how prac-
tical applications of interpretable AI depend on spe-
cific formal properties of interpretable models – in
this case monotonicity and linear additivity.
The proposed method for generating linguistic ex-
planations has been tested and refined through a de-
sign workshop with orthopaedic surgeons. Overall,
the findings from the workshop yielded generally pos-
itive feedback. Nevertheless, the extent to which the
explanations meet needs of doctors and patients in
real-world clinical settings has not been studied. In
a planned next step, the approach will therefore be
tested in a clinical study, where interactions between
patient, doctor, and predictive tool will be recorded
and analysed. Doctors’ and patients’ experiences of
using the tool will also be investigated through inter-
views and questionnaires.
In future work, it might also be useful to conduct
a more fine-grained argumentation analysis with all
Toulmin’s (Toulmin, 2003) argumentative elements
(e.g. backing and qualifier). Moreover, in the cor-
pus analysis it was observed that claims and their ac-
companying data/warrants might be complex in that
they are structured with one argument element em-
bedded in another, having a coordinative arrangement
or other potential arrangements (see, e.g. (Eemeren
et al., 2021)). More elaborate annotation will be re-
quired to bring out these forms of structuring and de-
termine their potential relevance in relation to model
interpretability and AI explanations.
6 ETHICS STATEMENT
Approval from the Swedish Ethical Review Author-
ity was obtained (case number 2024-00839-01) for
handling (de-identified) patient data from Swespine’s
registry. The Ahus data has previously been collected
with informed consent and stored in anonymized form
in accordance with approval from the Regional Ethics
Committee for Medical Research (Gulbrandsen et al.,
2013); since the data is anonymized, no ethical ap-
proval in Sweden was needed for using the data for
the present study.
ACKNOWLEDGEMENTS
The authors would like to thank the anonymous re-
viewers for useful comments and suggestions. This
work was supported by the Swedish Research Coun-
cil (VR) grant 2014-39 for the establishment of the
Centre for Linguistic Theory and Studies in Probabil-
ity (CLASP) at the University of Gothenburg.
REFERENCES
Ahmed, S., Shamim Kaiser, M., Hossain, M. S., and An-
dersson, K. (2024). A Comparative Analysis of LIME
and SHAP Interpreters with Explainable ML-Based
Diabetes Predictions. IEEE Access, pages 1–1.
From Interpretability to Clinically Relevant Linguistic Explanations: The Case of Spinal Surgery Decision-Support
919

Alonso, J. M. and Bugar
´
ın, A. (2019). ExpliClas: Au-
tomatic Generation of Explanations in Natural Lan-
guage for Weka Classifiers. In 2019 IEEE Interna-
tional Conference on Fuzzy Systems (FUZZ-IEEE),
pages 1–6. IEEE.
Baaj, I. (2022). Explainability of possibilistic and fuzzy
rule-based systems. Theses, Sorbonne Universit
´
e.
Berman, A. (2024a). Argumentative Dialogue As Basis For
Human-AI Collaboration. In Proceedings of HHAI
2024 Workshops.
Berman, A. (2024b). Too Far Away from the Job Mar-
ket – Says Who? Linguistically Analyzing Rationales
for AI-based Decisions Concerning Employment Sup-
port. Weizenbaum Journal of the Digital Society, 4(3).
Breitholtz, E. (2020). Enthymemes and Topoi in Dialogue:
the use of common sense reasoning in conversation.
Brill.
Eemeren, F. H., Garssen, B., and Labrie, N. (2021). Argu-
mentation between Doctors and Patients. Understand-
ing clinical argumentative discourse. John Benjamins
Publishing Company.
Forrest, J., Sripada, S., Pang, W., and Coghill, G. (2018).
Towards making NLG a voice for interpretable ma-
chine learning. In Proceedings of The 11th Interna-
tional Natural Language Generation Conference. As-
sociation for Computational Linguistics (ACL).
Fritzell, P., Mesterton, J., and Hagg, O. (2022). Prediction
of outcome after spinal surgery—using The Dialogue
Support based on the Swedish national quality regis-
ter. European Spine Journal, pages 1–12.
Grice, H. P. (1975). Logic and conversation. Syntax and
semantics, 3:43–58.
Gulbrandsen, P., Finset, A., and Jensen, B. (2013). Lege-
pasient-korpus fra Ahus.
Kaczmarek-Majer, K., Casalino, G., Castellano, G., Do-
miniak, M., Hryniewicz, O., Kami
´
nska, O., Vessio,
G., and D
´
ıaz-Rodr
´
ıguez, N. (2022). Plenary: Explain-
ing black-box models in natural language through
fuzzy linguistic summaries. Information Sciences,
614:374–399.
Lindgren, S. and Aspegren, K. (2004). Kliniska f
¨
ardigheter:
informationsutbytet mellan patient och l
¨
akare. Stu-
dentlitteratur AB.
Lundberg, S. M. and Lee, S.-I. (2017). A unified ap-
proach to interpreting model predictions. In Guyon, I.,
Luxburg, U. V., Bengio, S., Wallach, H., Fergus, R.,
Vishwanathan, S., and Garnett, R., editors, Advances
in Neural Information Processing Systems 30, pages
4765–4774. Curran Associates, Inc.
Maraev, V., Breitholtz, E., Howes, C., and Bernardy, J.-
P. (2021). Why should I turn left? Towards active
explainability for spoken dialogue systems. In Pro-
ceedings of the Reasoning and Interaction Conference
(ReInAct 2021), pages 58–64.
Miller, T. (2019). Explanation in artificial intelligence: In-
sights from the social sciences. Artificial Intelligence,
267:1–38.
Miller, T. (2023). Explainable AI is Dead, Long Live Ex-
plainable AI! Hypothesis-driven Decision Support us-
ing Evaluative AI. In Proceedings of the 2023 ACM
Conference on Fairness, Accountability, and Trans-
parency, FAccT ’23, page 333–342, New York, NY,
USA. Association for Computing Machinery.
Pantanowitz, L., Pearce, T., Abukhiran, I., Hanna, M.,
Wheeler, S., Soong, T. R., Tafti, A. P., Pantanowitz,
J., Lu, M. Y., Mahmood, F., Gu, Q., and Rashidi,
H. H. (2024). Nongenerative Artificial Intelligence in
Medicine: Advancements and Applications in Super-
vised and Unsupervised Machine Learning. Modern
Pathology, page 100680.
Ribeiro, M. T., Singh, S., and Guestrin, C. (2016). ”Why
Should I Trust You?”: Explaining the Predictions
of Any Classifier. In Proceedings of the 22nd
ACM SIGKDD International Conference on Knowl-
edge Discovery and Data Mining, pages 1135–1144.
Rudin, C. (2019). Stop explaining black box machine learn-
ing models for high stakes decisions and use inter-
pretable models instead. Nature Machine Intelligence,
1(5):206–215.
Rudin, C., Chen, C., Chen, Z., Huang, H., Semenova, L.,
and Zhong, C. (2022). Interpretable machine learn-
ing: Fundamental principles and 10 grand challenges.
Statistics Surveys, 16(none):1 – 85.
Sbis
`
a, M. (1987). Acts of explanation: A speech act anal-
ysis. Argumentation: Perspectives and approaches,
pages 7–17.
Slack, D., Krishna, S., Lakkaraju, H., and Singh, S. (2023).
Explaining machine learning models with interactive
natural language conversations using TalkToModel.
Nature Machine Intelligence, 5(8):873–883.
Toulmin, S. E. (2003). The uses of argument. Cambridge
university press.
Wahde, M. and Virgolin, M. (2023). DAISY: An Implemen-
tation of Five Core Principles for Transparent and Ac-
countable Conversational AI. International Journal of
Human–Computer Interaction, 39(9):1856–1873.
Winograd, T. (1971). Procedures as a representation for
data in a computer program for understanding natu-
ral language. PhD thesis, Massachusetts Institute of
Technology.
Xydis, A., Hampson, C., Modgil, S., and Black, E. (2020).
Enthymemes in dialogues. In Computational Models
of Argument, pages 395–402. IOS Press.
IAI 2025 - Special Session on Interpretable Artificial Intelligence Through Glass-Box Models
920
