
Recommendations of Embodied Conversational Agents
to Healthcare Applications
Julio Oliveira
1a
, Telmo Silva
1b
Rita Oliveira
1c
and Elizabeth Furtado
2d
1
Digimedia, Universidade de Aveiro, Aveiro, Portugal
2
Doutorado em Informática Aplicada, Universidade de Fortaleza, Fortaleza, Brazil
Keywords: ECA, Embodied Conversational Agent, Hypertension, Older Adults.
Abstract: This paper identifies recommendations for Embodied Conversational Agents (ECA) in Healthcare
applications. The methodology employed consists of two systematic literature reviews in the fields of
conversational systems and health care. Twenty-six recommendations for ECA were categorized into four
groups: CS Interface, ECA Functionalities, Agent Behavior, ECA Customization Features, and Older Adults
Engagement. Additionally, six Healthcare dimensions were identified: Interactive Learning, Disease-Specific
Knowledge, Reinforcement, Emergency Detection, and Empathy/Rapport. These two sets of findings were
combined for evaluation by a group of experts. The impact evaluation revealed six essential, two necessary,
and eighteen desirable recommendations. The essential recommendations, derived from empirical methods,
include the following: storing encrypted information, providing secure and accurate information to patients,
facilitating interactive learning, allowing users to choose whether to enable proactive mode and ensuring ease
of installation and use. The set of recommendations is an important contribution for ECA developers as this
research presents.
1 INTRODUCTION
The use of Conversational Systems – CS in health
care is not recent. The first CS was ELIZA, developed
by Weizenbaum, and evolved from a simple chatbot
to multimodal communication (Car et al., 2020). CS
can be interactive, use active two-way
communication, and use speech as a method of
communication with the patient. The technology can
suit various populations, ranging from young children
to older people.
The use of CS can promote effective interaction,
engagement, and intervention, particularly in
managing chronic conditions, promoting healthy
behaviour, and supporting older adults (Pradhan et
al., 2020). Special Conversational Agents allow
reliable and efficient information delivery and should
exhibit social skills (Yang & Aurisicchio, 2021).
These skills include using nonverbal behaviour to
convey communicative and social signals. Ideally,
a
https://orcid.org/0000-0002-3516-0114
b
https://orcid.org/0000-0001-9383-7659
c
https://orcid.org/0000-0001-6041-9469
d
https://orcid.org/0000-0002-1584-3161
agents should be able to produce and recognize
nonverbal signals in simulations of face-to-face
actions. Agents with such capabilities are named
Embodied Conversational Agents - ECA (Barros,
2021, Bickmore & Cassell, 2005). Some features
related to ECA are facial and body expressions,
movement of parts, and even the use of lights and
colors to promote interaction (Potdevin et al., 2021;
Ruttkay et al., 2004).
From the perspective of ECA´s development,
features, recommendations, characteristics, and
emphatic aspects need to be related to Health Care.
There are a lot of existing recommendations in
Literature, but we propose a way to validate them
using a questionnaire with specialists. The result is a
list of recommended features to achieve healthcare
support and coaching. This under-progress work is a
part of PhD Thesis and intends to identify the
recommendations for the use of ECA in support of
hypertension treatment by Older Adults.
352
Oliveira, J., Silva, T., Oliveira, R. and Furtado, E.
Recommendations of Embodied Conversational Agents to Healthcare Applications.
DOI: 10.5220/0013438700003938
In Proceedings of the 11th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2025), pages 352-359
ISBN: 978-989-758-743-6; ISSN: 2184-4984
Copyright © 2025 by Paper published under CC license (CC BY-NC-ND 4.0)
The next section presents material and methods
used to collect the recommendations and key aspects
of Health. Section three presents twenty-six ECA
recommendations grouped by their functions. The
fourth section presents six key dimensions of Health
Care as a parameter to combine with ECA´s
recommendations. Section five shows the results of
matching the two sets of Recommendations and Key
Dimensions of Health found. The last section
proposes future works.
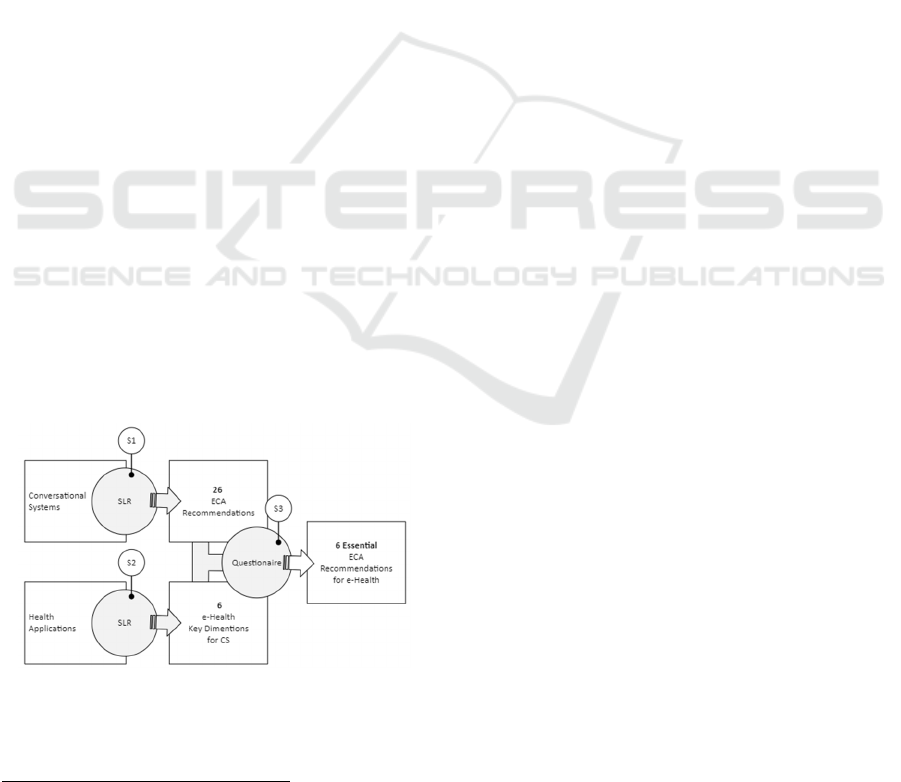
2 MATERIAL AND METHODS
Two Systematic Literature Reviews (SLRs) and
questionnaires were used to identify the ECA
recommendations. The process was made in three
steps, as shown in Figure 1.
The first Step (S1) was a SLR with the query
“("evaluation of" OR "guidelines" OR "heuristics"
OR "recommendations”) AND ("embodied" OR
"conversational Agents" OR "voice Agents") AND
("elder*" OR “senior" OR "older adults")”.
The Scopus
1
database returned six articles, and the
ACM Digital Library database, 33 articles, totalling
39 sources to be analyzed. After reading the abstracts,
29 were eliminated: 12 that were not related to the
ECA in Health Care, five did not involve ECAs, 8 did
not involve older adults, two dealt with text interfaces
(chatbots), in addition to 2 repeated articles. After the
full reading of the articles, five were selected, which
will be summarized in the next section. The update
phase included more three papers considering the
actual stage of the Large Language Model (LLM),
such as ChatGPT. From the reading 26 ECA
Recommendations were listed to be used in Step 3.
Figure 1: Steps to Identify Essential Recommendations
ECA in Health Care (created by the author).
1
Scopus Database. Available Sep 11, 2024,
https://www.scopus.com
The SLR made in Second Step (S2) used the
query “("e-health" OR "health" OR "telemedicine")
AND ("recommendation" OR "dimension*") AND
("voice") AND ("embodied" OR "conversational
Agents" OR "Conversational System" AND "older
adults" AND NOT "mental health") excluding
publications before 2022. Scopus returned five papers
and ACM Library 35 publications. 32 were
eliminated: 10 that did not involve ECA and Health
Care, 12 did not present any recommendation for
Health use, and obtained 8 articles. Six key
dimensions were selected to play the role of
evaluating each ECA´s recommendation identified.
The final step (Step 3) investigates the ECA
Recommendations concerning the Key Dimensions
found and their importance in achieving effective
Health Care. The method used was a digital
questionnaire to eight experts in Conversational
System applied to e-Health. The results found are
detailed in section five.
3 ECA RECOMMENDATIONS
In this work, an ECA Recommendation is a guideline
related to the CS Interface, ECA Functionalities,
Agent Behavior, or ECA Customization Features.
Each author presents suggestions for the features or
characteristics of an ECA. Six design
recommendations of ECA for interaction with elderly
people with dementia were extracted from EVA
conversational agent from EVA conversational agent
(Sandoval & Favela, 2017).
ECA LOUISE presented Alternatives to
overcome the user interface restrictions linked to
cognitive impairment in the elderly, making it
possible to establish 14 recommendations (Wargnier
et al., 2018). Eleven recommendations were
identified in the results presented in a Systematic
Mapping Study of Usability and User eXperience of
CS (Guerino & Valentim, 2020).
There are 13 guidelines presented in a study that
involves older people with dementia identified in a
Voice User Interface (VUI) development (Striegl et
al., 2021a). Of the 44 recommendations A total of 18
recommendations were excluded due to the repetition
of features. The remaining 26 recommendations were
systematically numbered to reference each type. Each
recommendation is tagged according to its
corresponding group: R1?? pertains to CS Interface,
R2?? relates to ECA Functionalities, R3?? addresses
Recommendations of Embodied Conversational Agents to Healthcare Applications
353
Agent Behaviour, and R4?? corresponds to
Customization Features, with ?? representing a
sequential number. The author has proposed a
classification system for the recommendations within
each group.
3.1 Recommendations on the CS
Interface
Table 1 identifies three Recommendations for the
Conversational System (CS) Interface. These
recommendations are proposed by (Wargnier et al.,
2018) and (Guerino & Valentim, 2020) and can be
applied to most ECA for health areas or others.
Recommendation R101 refers to the need for
adjustments after the first use of ECA. At this point,
the input phrase should be indicated and, if possible,
modified (R102). Recommendation R103 highlights
the ease of use of ECA for users who are not familiar
with the technology. The configurations, such as
connection to the network, must be made by an initial
dialog.
Table 1: Recommendations on the CS Interface.
Conversational S
y
stem Interface
(
R101
)
Sim
p
le interface, no learnin
g
re
q
uire
d
(
R102
)
Indicate the A
g
ent's entr
y
p
h
r
ase
(R103) Agents should be ready to use immediately.
3.2 ECA Functionalities
Ten recommendations related to Conversational
System functionalities are listed in Table 2.
Recommendation R201 is related to the use of
external sensors such as the User´s temperature and
heartbeat, brain activities, and emotional responses
from the skin. Those sensors generally reduce the
usability of the equipment as they use wires to
connect the users to the ECA.
Recommendations R202 - Recognize the
environment of use and R203 - Recognize the user by
speech (Riccardi, 2014) requires a camera and
microphone connected to the ECA to assess the
environment and record the user's voice. These
recordings and further information must attend the
R204 and be encrypted to give maximum security and
privacy to the user data. Recommendations R205 -
Track the user and R206 - Locate the sound source
proposed by (Wargnier et al., 2018) are met when
more than one microphone is installed. Sound
localization in artificial systems usually uses two (or
more) microphones. By the difference in the arrival
times of a sound of the microphones, it is possible to
estimate the direction of the sound source
mathematically.
For the user to see realistic lip-synchronization
movements with speech, expressive feedback in
speech, and gestures, virtual agents need to use real
graphical animations for the user: R207 - Introduce
advanced features in avatar animation (Striegl et al.,
2021).
Recommendation R208 - Provide secure and
correct information is a feature linked to the base of
knowledge accessed by the ECA. A (medical) team
must validate the source of information. In a case of
doubt, the ECA must send the issue to a human. Once
the human team has defined the procedure to be taken
and the answer to be given, it should input it into the
knowledge base (R209: Provide learning) (Striegl et
al., 2021).
The last recommendation in this group deals with
storing the dialogues that have already been taken
with the user. Further communication can use the
previous information to provide a real human dialog.
The greatest care taken with this recommendation lies
in identifying true and doubtful information. The
process of filtering out errors must be planned to
make the result relevant (R210: Provide continuity in
dialogue).
Table 2: Recommendations for ECA Functionalities.
ECA Functionalities
(R201) Recognize embedded signals (Use of sensors)
(R202) Recognize the environment of use
(R203) Recognize the user by speech
(R204) Store encrypted information
(R205) Track the user
(R206) Locate the sound source
(R207) Introduce advanced features in avatar animation
(R208) Provide secure and correct information
(R209) Provide learning
(R210) Provide continuity in dialogue
3.3 Agent Behaviour
Recommendations
This group recommendation is related to the
Behaviour of the Conversational Agent itself. The six
recommendations are listed in Table 3 and explained
as follows. The agent must incorporate the ability to
coordinate and regulate emotions and understand the
affective sustainability of interaction with ECA
(R301: Contemplate affectivity).
To perform a (R302 Allow Sociability) “(..) Not
only must a Virtual Agent be able to understand the
user's emotion, but they must also be able to respond
accordingly" (Riccardi, 2014). This social component
is a key human skill and will be a research challenge
ICT4AWE 2025 - 11th International Conference on Information and Communication Technologies for Ageing Well and e-Health
354
for human-machine interaction and possibly for
machine-machine interaction (Riccardi, 2014).
Recommendation R303 - Contemplate the avatar's
Behavioural reaction, established by (Wargnier et al.,
2018), relates to implementing a behaviour analysis
module based on recommendations R203, R206,
R207, and R208 described in item 3.1.2.
Recommendation R304 - Assist the user as little
as necessary refers to the ability of communicate to
the user in different ways, depending on the dialog.
This feature is necessary to include people who does
not understand easily an instruction (Striegl et al.,
2021b). The R305 Track the user's progress during
the execution of a task is related to R205 but is not the
same. This recommendation refers to tracking the
user's body and face when executing a task.
The last recommendation of this group is R306 -
React autonomously to user requests. The agent needs
to be aware of a call and react not only with voice but
with non-verbal activity such as a voice change or
intonation.
Table 3: Agent Behaviour Recommendations.
A
g
ent Behaviour
(R301) Contemplate affectivity
(R302) Allow Sociability
(R303) Contemplate the avatar's Behavioural reaction;
(R304) Assist the user as little as necessary, breaking
down complex instructions based on the needs of
the users
(R305) Track the user's progress during the execution
of a task
(R306) React autonomously to user requests
3.4 ECA Customization Features
The Recommendations group related to customization
and configuration are outlined in
Table
4. The first recommendation refers to the
proactiveness of ECA (R401). Proactive engagement,
such as medication adherence and health monitoring
reminders, enhances the utility of ECAs. Interactive
elements foster continuous user participation, as
evidenced by studies on virtual agents like PACO and
Addison Care (Krutter et al., 2022). To perform user
security, the ECA must attend the R401 - provide
control and adjustments in interventions from the
ECA with the user. If the interventions of the ECA
could be made without the Entry Phrase, the user must
allow the record of all sounds around the equipment.
The interventions must be realized without user
command to permit a proactive comportment.
The second recommendation of this group is
R402, which refers to the adjustment of personality,
conversation topics, or vocabulary according to the
user. This allows the user to configure the personality
of the Agent, such as the way of abord themes, for
example. Also, the conversation topics, in our case
the Health field, and mainly a vocabulary depending
on the user's level of knowledge (Guerino &
Valentim, 2020). The recommendation numbered by
R403 provides a way to configure different faces,
voices, gestures, and embedding. Adjustment of the
ECA Agent is a key to improve empathy with the
user. The level of configuration starts from the gender
of the agent and can be personalized to a real human
characteristic. A work draws attention to the fact that
the customization of the pronunciation and
personality of the agent is not indicated (Guerino &
Valentim, 2020).
Recommendation R404 refers to adding new
character models quickly; this feature is a way to
propose a known person as the agent.
Recommendation R405 is about to describe
interaction scenarios in a dedicated syntax. A way to
guide the user to some tasks is to adopt scenarios. In
this solution, the user can describe what the ECA
should do to achieve a goal. For example, the user
should ask the ECA to measure the blood pressure 3
times a day and inform any anomaly to medical
support. The personalization of the pronunciation of
the Agent voice (R406) refers to promoting different
voice intonation and word pronunciation. It is
remarkable when the same language is spoken in
countries like Portugal and Brazil. For example, the
agent's voice must be configurable to Portuguese of
Portugal residents.
Table 4: Recommendations for Agent Customization.
ECA Personalization
(R401) Allows control and adjustments in interventions
(R402) Allows adjustment of personality, conversation
topics, or vocabulary according to the user
(R403) Allows to configure different faces, voices,
gestures, and embedding
(R404) Allows to add new character models easily;
(R405) Describe interaction scenarios in a dedicated
syntax
(R406) Personalize the pronunciation of the agent voice
(R407) Set up the entry phase, response times, speed
and speaking style
Besides, pronunciation is necessary to configure
the tone, velocity, and other voice characteristics, such
as an agitated woman's voice or an old, relaxed voice
(R407). This fine configuration of the Avatar
communication is fundamental to an effective human-
like dialog experience. The goal is to perform
comfortable and easy-to-understand communication
between the agent and the user. The configuration
Recommendations of Embodied Conversational Agents to Healthcare Applications
355

must be made easily, giving the user alternatives to
choose or recording an example sample voice to be
used.
4 HEALTHCARE DIMENSIONS
Healthcare has shown a particular interest in the use of
Conversational Agents such ECA (terStal et al., 2020).
To develop the ECA to support eHealth areas, it is
necessary to discover mandatory ECA
recommendations to achieve better patient
engagement.
Technology variability of CS is related to nine
aspects: devices, application technology, service
channel, hosting and storage, electronic health record
(EHR) integration, input/output model, intelligence
framework, sentiment detection, and privacy and
security (May & Denecke, 2024).
User-related variability is related to seven aspects:
human involvement, care flow integration, patient
profile, language and communication style, health
literacy, service duration, and personal preference
(May & Denecke, 2024).
The listed variables were mapped into six
dimensions: Interactive Learning, disease-specific
Knowledge, Reinforcement, Emergency Detection,
and Empathy/Rapport.
4.1 Interactive Learning
In an Interpretative Model of Interaction by Patient-
Physician (Gross et al., 2021) the Physician interprets
the patient's values, and the patient decides.
Using an ECA as the physician is necessary for an
Interactive Learning (IL) approach to engage and
educate patients about health topics (Egede et al.,
2021). The method should use videos, graphics, and
animations to illustrate the concepts and show
examples. The IL needs to be applied to Health
Literacy and all engaging procedures like medicine
intake, treatment procedures, alimentary suggestions,
and so on.
4.2 Disease-Specific Knowledge
Disease-Specific Knowledge (SK) refers to the ECA
performing accurate and up-to-date information on
specific. The outcome of the health system is to
provide correct information depending on the patient,
based on the EHR. (Egede et al., 2021).
Some conversational systems, such as Alexa or
Google Assistant, use the Internet as a source of
knowledge. This dimension points to a dedicated
base created by specialists.
4.3 Reinforcement
The Reinforcement (R) is a feature related to
repeating messages over time until the goal is
obtained. To follow a treatment or a medicine
administration, the patient needs to be aware several
times (Egede et al., 2021). Reinforcement learning is
a technique involving an agent who needs to decide
which actions it needs to do to perform a task that has
been assigned to it most effectively. For this, rewards
are assigned to the different actions that the agent can
take in different situations or states of the
environment.
Initially, the agent has no idea about the best or
correct actions. Using reinforcement learning, it
explores its action choices via trial and error and
figures out the best set of actions for completing its
assigned task. The basic idea behind a reinforcement
learning agent is to learn from experience. Just like
humans learn lessons from their past successes and
mistakes, reinforcement learning agents do the same
– when they do something “good,” they get a reward,
but if they do something “bad”, they get penalized.
The reward reinforces the good actions while the
penalty avoids the bad ones.
Reinforcement learning requires several key
components: Agent – This is the “who” or the subject
of the process, which performs different actions to
perform a task that has been assigned to it.
Environment – This is the “where” or a situation in
which the agent is placed. Actions – This is the
“what” or the steps an agent needs to take to reach the
goal. Rewards – This is the feedback an agent
receives after performing an action.
4.4 Emergency Detection
To allow the user a way to Emergency Detection
(ED), which refers to the ability to recognize and
respond to potential health emergencies (Sunghoon et
al., 2019). Specialized sensors can detect alterations
in the health state of the patient. Such sensors are
electrocardiogram sensor (ECG), Electromyography
(EMG), Electro dermal Activity (EDA), or
Accelerometer sensor (ACC). Cameras and
microphones can, otherwise, help to identify some
emergencies in conversational voice systems. This
feature can give the patient a way to have care even if
he/she is not conscious or cannot move.
ICT4AWE 2025 - 11th International Conference on Information and Communication Technologies for Ageing Well and e-Health
356
4.5 Empathy and Rapport
The Empathy and Rapport (ER) of a conversational
system uses a psychological approach to simulate a
human interaction. Features like mirroring verbal and
nonverbal Behaviours, providing contextually
appropriate emotional expressions, and maintaining
continuity in dialogue have improved patient
outcomes in medical systems(Salman et al., 2021,
2023).
5 RESULTS
To identify the essential recommendations that ECA
needs to contemplate in a Health Care application for
treatment support in older adults, we made an
empirical study. This holistic approach can be used to
deploy an ECA or evaluate an existing one. We start
by matching each dimension described in Section 4
with the recommendations of Section 3. This process
was made by the author and is listed in Table 5. Some
recommendations did not match any Health Care Key
Dimensions and were classified as General (G) ECA
Recommendations.
After the match, a questionnaire was elaborated in
Portuguese to identify the impact of each
recommendation on each dimension. The
questionnaire was submitted to 2 developers of ECA
to support patients, three UX specialists, a Portuguese
nurse, and experts totaling eight participants.
For each Recommendation, the participants
indicate the ECA recommendation as Unnecessary:
The recommendation does NOT need to be in the
ECA to carry out activities to support the treatment of
diseases for older adults; Desirable: The
recommendation does not need to be in the ECA to
achieve the proposed objectives but can somehow
improve the engaging process; Necessary: The
recommendation is fundamental and Cannot
Evaluate: There is no consensus, or the text of the
recommendation is unclear.
The main finding is that no recommendation was
categorized as Unnecessary (Figure 2). This points
out that, somehow, all the guidelines contribute to
performing effective Health Care. The Desirable set
was the biggest one: 70% of the total. The related
health dimensions were Emergency Detection,
Empathy and Rapport, and all general dimensions.
Special sensors related to Emergency Detection are
set as Desirable as the devices are not easy to use and
install in patients. The participants wrote about the
difficulties related to considering these features as a
second round of testing. An effective Emergency
Detection Device needs to guarantee 100% free error.
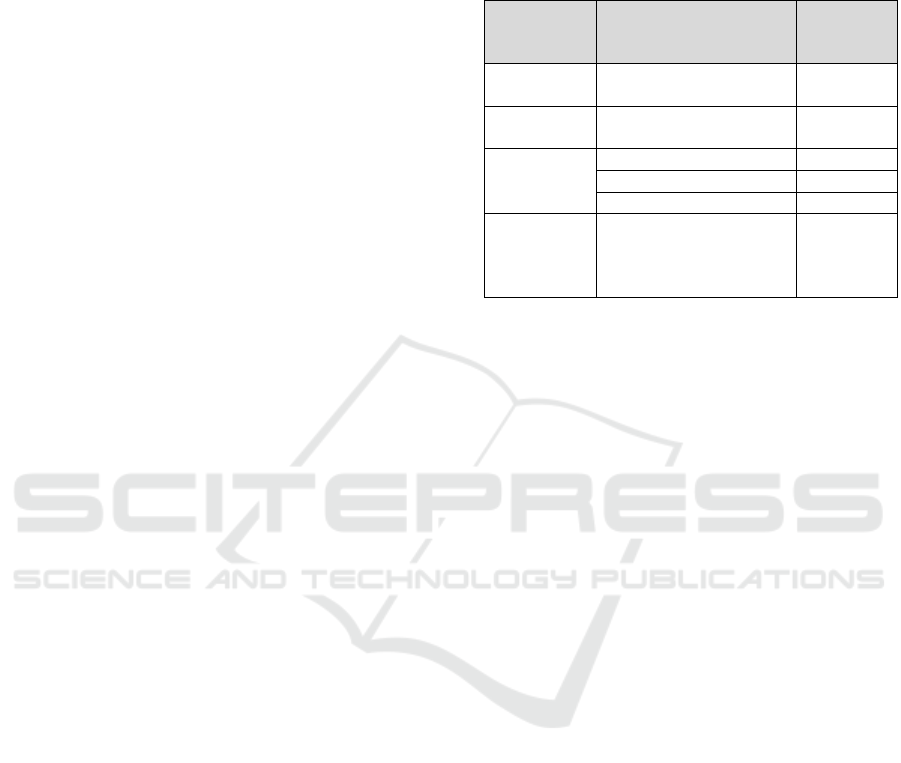
Table 5: Health Care Dimensions x ECA
Recommendations x Impact.
Health
Dimension
ECA
Recommendations
related
Impact
IL, SK, R R204, R208, R209 and
R210
Essential
ED R201, R202, R203,
R205, R206 and R305
Desirable
ER R103 and R401
E
ssential
R301 and R302
N
ecessar
y
R303 Desirable
General R101, R102, R207,
R304, R306, R402,
R403, R404, R405,
R406, R407
Desirable
Another recommendation set as Desirable was
R303, Contemplate the avatar's Behavioural reaction.
The respondents complain about the complexity of
non-verbal feedback. This recommendation is related
to the other General Recommendations, including
R402, which allows adjustment of personality,
conversation topics, or vocabulary according to the
user, and R403, which allows the configuration of
different faces, voices, gestures, and embedding.
Although the configuration set recommendations
are important to an ECA, the participants evaluate
them as desirable. This fact needs to be revisited in
future works to validate them.
There were two Necessary recommendations:
R301, contemplate affectivity, and R302, Allow
Sociability. They are concerned with the dialog
between the ECA and the user. The Agent needs to
incorporate empathic and motivational dialogues and
enhance user adherence. To confirm this, empathic
dialogue frameworks based on doctor-patient
communication inspire design principles that make
ECAs more relatable and supportive (Salman et al.,
2021). The R401 is mainly about a proactive feature
of the ECA.
Related to Interactive Learning, disease-Specific
Knowledge and Reinforcement were identified as 4
Essential Recommendations. The R204
Recommendation is related to storing encrypted
information and guaranteeing the ethical aspects of
the health field. Recommendation R208 is as
important as the previous one as it provides secure
and correct information to the patient. There are no
cues to errors when health treatments involve
recommendation R209 to provide learning from the
doctor team. The learning phase must be carefully
Recommendations of Embodied Conversational Agents to Healthcare Applications
357

planned to prevent any misunderstanding in the
dialog. R210 is concerned about the continuity of the
dialogue. This feature is necessary to prevent the user
from repeating or forgetting information.
Two essential recommendations related to
empathy and rapport were identified: R103, which is
related to the immediate use of the agents, and R401,
which allows the user to control and adjust
interventions and prevent proactiveness, for example.
6 CONCLUSION
The Recommendations encompass various aspects,
including user interface design, agent behavior, and
customization features, all aimed at improving user
experience and engagement. The findings underscore
the importance of incorporating social skills and
nonverbal communication into ECAs, which are
essential for fostering empathetic interactions and
enhancing the overall effectiveness of these systems
in healthcare settings.
Moreover, the empirical study conducted to assess
the impact of ECA recommendations on healthcare
dimensions highlights the necessity of aligning
technological capabilities with user needs. The results
indicate a set of essential recommendations
contribute to effective healthcare delivery, with a
significant proportion categorized as desirable
(Figure 2). This suggests that while certain features
may not be immediately essential, they can enhance
user engagement and satisfaction, ultimately leading
to better health outcomes.
The emphasis on proactive features and the ability
to adjust interventions further illustrates the need for
ECA to be adaptable to individual user preferences
and requirements.
In conclusion, developing and implementing
ECAs in healthcare represents a promising avenue for
improving patient support and engagement. By
adhering to the identified recommendations and
focusing on user-centered design, healthcare
providers can leverage the capabilities of ECAs to
create more effective and empathetic interactions.
Future research should continue to explore the
nuances of ECA.
7 FUTURE WORK
The SLR conducted in this study reveals a
comprehensive set of recommendations for the design
and functionality of ECAs tailored for healthcare
applications. The use of such methodology can be
complemented with a LLM search to complete the
study. Relating the ECA recommendations to health
apps mostly involved developers and UX specialists.
Figure 2: ECA Recommendations (by the author).
It is necessary to revisit these findings with doctors,
nurses, and patients to validate all finds registered.
This is the next step of the work and will be made in
Portugal and Brazil with older adults.
To complete the study, it is necessary to
investigate suggestions made by the respondents in
the questionnaire related to section five. Some of the
• Agents should be ready to use
immediately (R103)
•Store encrypted information (R204)
•Provide secure and correct information (R208)
•Provide learning (R209)
•Provide continuity in dialogue (R210)
•Allows control and adjustments in
interventions (R401)
Essencial
• Contemplate affectivity (R301)
• Allow Sociability (R302)
Necessary
• Simple interface, no learning required (R101)
• Indicate the Agent's entry phrase (R102)
•Recognize embedded signals (Use of sensors)
(R201)
•Recognize the environment of use (R202)
•Recognize the user by speech (R203)
•Track the user(R205)
•Locate the sound source(R206)
• Introduce advanced features in Agent
animation (R207)
•Contemplate the avatar's Behavioural reaction
(R303)
• Assist the user as little as necessary (R304)
• React autonomously to user requests (R306)
• Contemplate adjustment of personality,
conversation topics, or vocabulary according to
the user (R402)
• Contemplate to configure different faces,
voices, gestures, and embedding (R403)
• Contemplate to add new Agent models
easily (R404)
•Contemplate interaction scenarios in a
dedicated syntax (R405)
• Personalize the pronunciation or personality
of the Agent (R406)
• Set up response times, speed and speaking
style, user name, and reminders (R407)
Desirable
ICT4AWE 2025 - 11th International Conference on Information and Communication Technologies for Ageing Well and e-Health
358

participants wrote about the recommendations and
the health aspects. Some related to the agent of ECA
itself and some to the health issues. At this stage, the
work is intended to serve as a basis for identifying the
characteristics that the agent must have to guarantee
user engagement with the ECA.
REFERENCES
Barros, M. I. T. (2021). Operacionalização de Técnicas de
Mudança Comportamental em Agentes
Conversacionais [Master]. Universidade de Lisboa.
Bickmore, T. W., & Cassell, J. (2005). Social Dialogue with
Embodied Conversational Agents. 23–54.
https://doi.org/10.1007/1-4020-3933-6_2
Egede, J., Trigo, M. J. G., Hazzard, A., Porcheron, M.,
Bodiaj, E., Fischer, J. E., Greenhalgh, C., & Valstar, M.
(2021). Designing an Adaptive Embodied
Conversational Agent for Health Literacy. Proceedings
of the 21th ACM International Conference on
Intelligent Virtual Agents, 112–119.
https://doi.org/10.1145/3472306.3478350
Gross, C., Schachner, T., Hasl, A., Kohlbrenner, D.,
Clarenbach, C. F., Wangenheim, F. V., & Kowatsch, T.
(2021). Personalization of conversational agent-patient
interaction styles for chronic disease management: Two
consecutive cross-sectional questionnaire studies.
Journal of Medical Internet Research, 23(5).
https://doi.org/10.2196/26643
Guerino, G. C., & Valentim, N. M. C. (2020). Usability and
User eXperience Evaluation of Conversational
Systems: A Systematic Mapping Study. ACM
International Conference Proceeding Series, 427–436.
https://doi.org/10.1145/3422392.3422421
Krutter, S., Schuessler, N., Kutschar, P., Šabić, E.,
Dellinger, J., Klausner, T., Nestler, N., Beasley, M., .
(2022). Piloting of the virtual telecare technology
Addison Care’ to promote self-management in persons
with chronic diseases in a community setting: protocol
for a mixed-methods user experience, user engagement
and usability pilot study. BMJ Open, 12(9).
https://doi.org/10.1136/bmjopen-2022-062159
May, R., & Denecke, K. (2024). Conversational Agents in
Healthcare: A Variability Perspective. ACM
International Conference Proceeding Series, 123–128.
https://doi.org/10.1145/3634713.3634717
Potdevin, D., Clavel, C., & Sabouret, N. (2021). Virtual
intimacy in human-embodied conversational agent
interactions: the influence of multimodality on its
perception. Journal on Multimodal User Interfaces,
15(1), 25–43. https://doi.org/10.1007/S12193-020-
00337-9/FIGURES/6
Pradhan, A., Lazar, A., & Findlater, L. (2020). Use of
intelligent voice assistants by older adults with low
technology use. ACM Transactions on Computer-
Human Interaction, 27(4).
https://doi.org/10.1145/3373759
Riccardi, G. (2014). Towards Healthcare Personal Agents.
RFMIR 2014 - Proceedings of the 2014 ACM
Roadmapping the Future of Multimodal Interaction
Research Including Business Opportunities and
Challenges, Co-Located with ICMI 2014, 53–56.
https://doi.org/10.1145/2666253
Ruttkay, Z., Dormann, C., & Noot, H. (2004). Embodied
Conversational Agents on a Common Ground (pp. 27–
66). Springer, Dordrecht. https://doi.org/10.1007/1-
4020-2730-3_2
Salman, S., Richards, D., & Caldwell, P. (2021). Analysis
of Empathic Dialogue in Actual Doctor-Patient Calls
and Implications for Design of Embodied
Conversational Agents. Italian Journal of
Computational Linguistics, 7(1 | 2), 91–112.
https://doi.org/10.4000/ijcol.862
Salman, S., Richards, D., & Dras, M. (2023). Identifying
Which Relational Cues Users Find Helpful to Allow
Tailoring of e-Coach Dialogues. Multimodal
Technologies and Interaction, 7(10).
https://doi.org/10.3390/mti7100093
Sandoval, D. C., & Favela, J. (2017). Co-designing
ambient-assisted interventions using digital
interlocutors for people with dementia. Proceedings of
the 2017 ACM International Joint Conference on
Pervasive and Ubiquitous Computing and Proceedings
of the 2017 ACM International Symposium on
Wearable Computers, 813–821.
https://doi.org/10.1145/3123024.3125615
Striegl, J., Gollasch, D., Loitsch, C., & Weber, G. (2021a).
Designing VUIs for Social Assistance Robots for
People with Dementia. ACM International Conference
Proceeding Series, 145–155.
https://doi.org/10.1145/3473856.3473887
Striegl, J., Gollasch, D., Loitsch, C., & Weber, G. (2021b).
Designing VUIs for Social Assistance Robots for
People with Dementia. ACM International Conference
Proceeding Series, 145–155.
https://doi.org/10.1145/3473856.3473887
Sunghoon, K., Parasuraman, G. M., & Jaunbuccus, S.
(2019). Elderly Care Assistant: A Discreet Monitoring
Tool. Lecture Notes in Electrical Engineering, 561,
287–301. https://doi.org/10.1007/978-3-030-18240-
3_27
ter Stal, S., Kramer, L. L., Tabak, M., op den Akker, H., &
Hermens, H. (2020). Design Features of Embodied
Conversational Agents in eHealth: a Literature Review.
International Journal of Human Computer Studies.
https://doi.org/10.1016/J.IJHCS.2020.102409
Wargnier, P., Benveniste, S., Jouvelot, P., & Rigaud, A. S.
(2018). Usability assessment of interaction
management support in LOUISE, an ECA-based user
interface for elders with cognitive impairment.
Technology and Disability, 30(3), 105–126.
https://doi.org/10.3233/TAD-180189
Yang, X., & Aurisicchio, M. (2021). Designing
Conversational Agents: A Self-Determination Theory
Approach. Proceedings of the 2021 CHI Conference on
Human Factors in Computing Systems, 1–16.
https://doi.org/10.1145/3411764.3445445
Recommendations of Embodied Conversational Agents to Healthcare Applications
359
